Download
1 / 41
770 likes | 1.35k Vues
Monitoring and Evaluation: Maternal and Child Nutrition . Session Objectives. By the end of this session participants will be able to: Apply basic M&E concepts to maternal and child nutrition interventions Design and use M&E frameworks for nutrition programs

E N D
Session Objectives By the end of this session participants will be able to: • Apply basic M&E concepts to maternal and child nutrition interventions • Design and use M&E frameworks for nutrition programs • Identify nutrition interventions and common indicators for assessing their results • Describe M&E challenges of nutrition programs
Session Overview • The problem of malnutrition • Interventions and strategies • M&E frameworks for nutrition programs • Common indicators & data sources • M&E challenges
The Problem • Malnutrition contributes to over half of all child deaths, (60%) • Malnutrition is largely hidden, (mild, moderate, ?)
Importance of malnutrition as an underlying factor in under-five mortality in Ethiopian Children. Others Diarrheal Diseases Malnutrition 58% Perinatal Complications Acute Respiratory Infections Malaria Measles WHO ’98
Micronutrient deficiencies • Micronutrient deficiencies have severe consequences; • Iodine deficiency damages intellectual development, • 50% of pregnant women and 40-50% of children < 5 in developing countries are iron deficient, • VAD affects > 100 million children, and is responsible for as many as one out of every four child deaths in places with Vitamin A deficiency,
Nutrition and Development • Nutritional status is a key indicator of progress in attaining MDGs; • Eradicate extreme poverty and hunger (Goal 1), • Achieve universal primary education (Goal 2), • Promote gender equality and empower women (Goal 3), • Reduce child mortality (Goal 4), • Improve maternal health (Goal 5), • Combat HIV/AIDS, malaria and other diseases (Goal 6), • Ensure environmental sustainability (Goal 7), • Develop a global partnership for development (Goal 8)
#1. Poverty alleviation - an indicator is % children underweight #2. Primary education - benefits can accrue when nutrition and cognition are adequate #3. Gender equality- better nourished girls likely to stay in school longer #4. Child mortality - 60% associated with malnutrition #5. Maternal health - anemia, iodine deficiency, low BMI associated with health indicators #6. Infectious diseases and HIV AIDS- malnutrition worsens and makes them more susceptible to adverse outcomes Nutrition is Critical in Achieving MDGs
World Fit for Children Goals • Reduction of child malnutrition among children under five years of age by at least one third, with special attention to children under two years of age. • Achieve the sustainable elimination of iodine deficiency disorders by 2005 • Achieve the sustainable elimination of vitamin A deficiency by 2010 • Reduce the prevalence of anemia (including iron deficiency) by one third by 2010
Mother’s nutrition Complementary feeding Breastfeeding Vitamin A and iron Sick/severe cases Iodized salt Interventions Proven to Reduce Malnutrition When Linked with Health Services (Essential Nutrition Actions)
Monitoring and Evaluation Frameworks for Nutrition Programs
IR2.1 Increase awareness of households & other key audiences about desirable nutrition and health behaviors through multiple channels, e.g. ‘change agents’ IR2.2 Increase ownership and participation of community leaders and groups in monitoring health and nutrition services and behaviors IR2.3 Stronger links between health systems and communities Results Framework SO: Vulnerable families achieve sustainable improvement in the nutrition and health status of seven million women and children by 2008 IR1 Service providers improve quality & coverage of maternal and child health & nutrition services & key systems IR2 Communities sustain activities for improved maternal and child survival and nutrition IR1.1 Coordinate/converge services provided by the Dept. of social services (ICDS) and MOH, e.g. through Nutrition and Health Days, and Block planning IR1.2 Build capacity of service providers, supervisors and managers in the dept. of social services (ICDS) and MOH Source: Adapted from CARE/India INHP II, DAP II 2001-2006
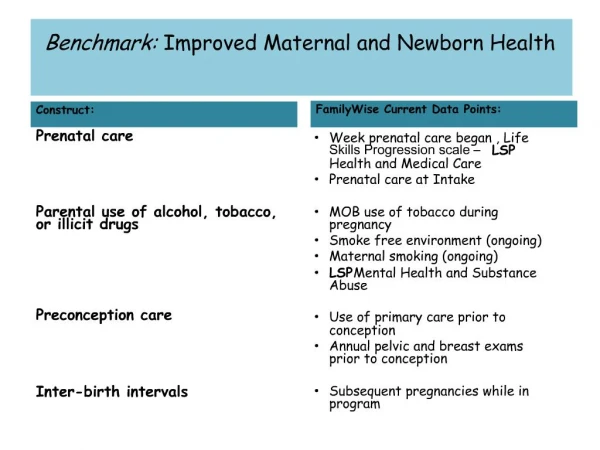
PURPOSE Sustainable improvement in the nutrition and health status of women and children through improved services provision and community participation PERFORMANCE INDICATORS 1.Proportion of children 6-35 months who are malnourished 2. Coverage of essential nutrition actions: exclusive BF, appropriate CF, vitamin A, iron supplements /fortified foods, iodized salt use, coverage of sick and malnourished in special programs 3. Proportion of households at risk of or vulnerable to food insecurity MEANS OF VERIFICATION 1.Annual reports from MCH services, special surveys 2.Annual reports, special surveys 3.National / local tracking reports (surveillance) of high risk areas/ populations ASSUMPTIONS - Stable political situation, sustained political commitment and financing - Sufficient numbers of competent health care personnel and supplies in the government sector - No natural disaster or disease epidemic Logical Framework NOTE: A logic model would allow a program to select indicators that monitor all stages (inputs, process, outputs) of their activities e.g. funds and staff available (inputs), training sessions completed (process), number of skilled workers or villages with trained volunteers (outputs).
Categories of Nutrition Indicators • Nutritional status • Breastfeeding practices • Complementary feeding practices • Micronutrient supplements/fortified foods • Household food security; vulnerability to food and nutrition insecurity
Most Common Indicators • Nutritional status • Weight-for-age and/or height-for-age • Body Mass Index in women • Anemia prevalence • Vitamin A deficiency • Infant and young child feeding practices • Timely initiation of breastfeeding • Exclusive breastfeeding rate • Complementary feeding rate • Extra feeding for malnourished/recently sick children
Most Common Indicators • Micronutrient Interventions • Vitamin A supplementation • Iron supplementation • Coverage with iodized salt, other fortified foods • Household Food Security/Vulnerability • Daily meal frequency of family/individuals • Perceived inadequacy of food reserves in the home/community
Data Collection Systems Routine • Sentinel food and nutrition surveillance • Institutional health records- clinics, schools • Feeding & cash or food transfer programs records- daily/weekly/monthly attendance Non-routine • Population-based surveys • Emergency appraisals, rapid assessments • Experimental and operational research
Anthropometric Measures (1) Children: • Weight-for-age (underweight) • Reflects chronic or acute malnutrition or both • Height-for-age (stunting) • Reflect chronic (prolonged, cumulative) malnutrition • Weight-for-height (wasting) • Reflects acute and recent malnutrition
Anthropometric Measurements (2) Adults: • Body Mass Index (BMI) • Low weight-for-height ( kg/m2) reflects chronic &/or acute • Mid-upper arm circumference (MUAC) • Thin reflects chronic &/or acute
Data Sources for Anthropometry • MCH programs/clinic records • School feeding- school heights. • Food and nutrition, epidemiological surveillance • Poverty mapping/school height census - heights for chronic, weights for current • Reports from emergency/refugee programs
Detecting Low Weight-for-age Option A Growth Chart Option B Table of weight-for-age cut-off points Cut-Off Points Low Weight-for-Age Girls Boys Age mths Age mths Low wt/age below this line Low wt for age below this line
Statistical Presentation of Anthropometric Indicators • Prevalence • Percent below a cut-off, such as <-2SD or < -3 SD • Mean Z-score values (in SD units) • Z score refers to how far and in what direction the measure deviates from the median of the NCHS/WHO international reference standard
Exercise: Interpreting Standard DHS Nutrition Status Tables • If low HFA is 50%, WFA is 30%, WFH is 15%, which is the worst problem? Why? • Which child is more vulnerable to die: a -sd wasted or a -3sd stunted child? Why? In which age group? • Which characteristics are more important for program targeting: rural/urban, region, sex, age, or birth order?
Feeding Practices: M&E Considerations • Proportion of infants aged 0-5 months who were exclusively breastfed in the last 24 hours, • Proportion of infants less than 12 months of age who were put to the breast within one hour of delivery, • Proportion of infants aged 6-9 months receiving breastmilk & complementary foods, • Mean number of food groups eaten in the last 24 hours by children 6-23 months of age,
Appropriate Complementary Feeding • Percentage of infants and young children 6 -23 months of age who receive appropriate complementary feeding • 6 to 8 months of age : Breastmilk + other food at least 2-3 times per day + variety of food groups • 9 to 11 months of age : Breastmilk + other food at least 3-4 times per day + variety of food groups • 12 to 23 months of age : Breastmilk + other food at least 3-4 times per day + variety of food groups
Coverage Indicators for Micronutrient Programs • Proportion of children aged 6-59 months who received a high dose of vitamin A in the last 6 months, • Proportion of households consuming adequately iodized (i.e. 15+ ppm of iodine) salt, • Proportion of pregnant women who received the recommended number of iron/folate supplements during pregnancy,
Choices in Program M&E Design • Which age groups to measure • Anthropometry, infant and young child feeding, • How to obtain valid measurements • Anthropometry; micronutrients; infant and young child feeding • Timing • Trends; seasonality • Evaluation design
Examples of Flaws in Nutrition Evaluations • No comparison groups • No pretest or baseline • No control for age, e.g. < 6 mo.,< 2 and 3+ yrs • Not accounting for confounding factors • Seasons not comparable • Not controlling for mortality reduction • Non-representative samples, small samples • Pilot projects, not replicable
Economic Analysis in Nutrition M&E • Cost-effectiveness analysis • compares two or more alternatives for achieving coverage or scale or behavior change, or a processoutcome such as training to build capacity • Answers the question ‘which is the more efficient option?’ • Used more in evaluations • Cost-benefit • compares the resources required to achieve impact and the monetary value of that impact • Answers the question ‘is the investment worthwhile?’ • Based on many assumptions with limited empirical evidence
Monitoring and Evaluation Challenges
Challenges of M&E • Multisectoral programs (attributing outcome?) • Clinical Indicators • May need large samples (e.g. xerophthalmia) • May be sensitive to enumerator training (e.g. goiter) • Measurement of iron deficiency (lack of specificity) • Selection bias (institution based sample)
Challenges: Comparisons & Trends • Sample design • Sample size • Cutoff points & standards • Seasonality
References • Arimond, Mary and Marie T. Ruel. 2003. Generating Indicators of Appropriate Feeding of Children 6 through 23 Months from the KPC 2000+. Washington, D.C.: Food and Nutrition Technical Assistance Project, Academy for Educational Development. • Cogill, Bruce. 2003. Anthropometric Indicators Measurement Guide. Washington, D.C.: Food and Nutrition Technical Assistance Project, Academy for Educational Development. • Wasantwisut, Emorn. 2002. Recommendations for monitoring and evaluating vitamin A programs: outcome indicators. Journal of Nutrition, 132: 2940S-2942S. • Ruel, M.T., K.H. Brown, and L.E. Caulfield. 2003. Moving Forward with Complementary Feeding: Indicators and Research Priorities. Food Consumption and Nutrition Division Discussion Paper #146. Washington, D.C.: International Food Policy Research Institute. • WHO. 2001a. Assessment of Iodine Deficiency Disorders and Monitoring their Elimination: A Guide for Programme Managers. Second Edition. WHO/NHD/01.1. Geneva: World Health Organization. • WHO. 2001b. Iron Deficiency Anaemia: Assessment, Prevention and Control - A Guide for Programme Managers. WHO/NHD/01.3. Geneva: World Health Organization. • Wellstart International’s Tool Kit for Monitoring and Evaluating Breastfeeding Practices and Programs.
Madagascar Nutrition Case Study During 1996-2002, Madagascar followed a comprehensive model, the “essential nutrition actions” (ENA) framework, which coordinated efforts from the community level through national policy making, and included both government and non-government entities. The model was first implemented in two districts in the Antananarivo and Fianarantsoa provinces. It focused on a set of proven interventions covering micronutrients and dietary practices for mother and young children. From 1995 to 1998, the overall focus was placed on designing mechanisms that linked nutrition interventions more directly with other child health and RH services, and national- and community-level actions. Further instructions are provided in the handout.