Download
1 / 12
140 likes | 862 Vues
Methods for Securing the Endotracheal Tube. Kitty Chan School of Nursing,The Hong Kong Polytechnic University Email: hskittyc@inet.polyu.edu.hk Date: 2003.

E N D
Methods for Securing the Endotracheal Tube Kitty Chan School of Nursing,The Hong Kong Polytechnic University Email:hskittyc@inet.polyu.edu.hk Date: 2003
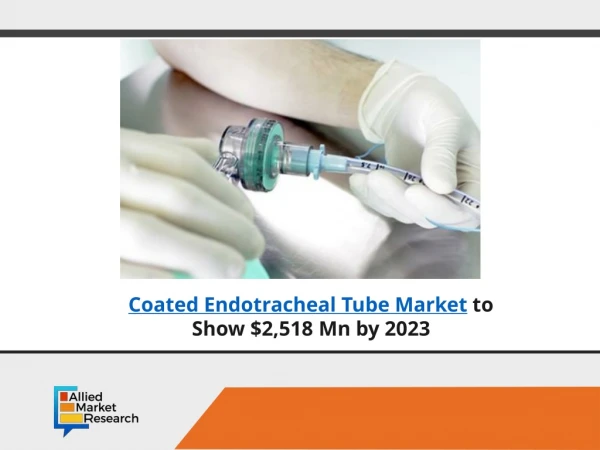
Various ways of securing the endotracheal tube (ETT) are available. This is important to prevent the ETT from being dislodged or displaced, leading to the ventilation of only one or neither of the lungs. The 3 main methods are by using adhesive tape, twill tape or commercial holders. The choice depends on the needs of the client and also on the institution standard. In this module, we demonstrate the use of the adhesive tape method and the use of twill tape when there is an abundance of oral secretions in the client, rendering it very difficult for the tapes to adhere. Methods for Securing the Endotracheal Tube
Use of Adhesive Tape • Prepare 2 long straps of Durapore. • To change ETT tapes, remove the old tapes & perform mouth care. Note any allergies to tape or ulcers.
Stabilize the ETT to avoid accidental extubation. An assistant may be required, particularly if the patient is restless. • Shift the ETT to the opposite corner of the mouth. Tape the first strap of Durapore as in the photo. Use of Adhesive Tape
Note position of the ETT where the marking should be at the incisor of the client. Use of Adhesive Tape • The tube is commonly placed at around 21-22 cm. • This should be the same as confirmed by CXR & documented in the patient’s chart.
Use of Adhesive Tape • Wrap the tapes around the ETT. • Both ends should be to one side of the mouth with this piece of tape; vice vera for the second piece of strap (as in this demonstration) • OR 2 ends at the opposite side of the mouth & the same for the second piece of tape.
Use of Twill Tape • Prepare the twill tape (cotton tape). • Double the tape & tie it around the ETT. • Pull the frayed ends to tighten the loop around the ETT.
Use of Twill Tape • Pull the 2 ends of the tape in opposite directions & tie a secure knot.
Use of Twill Tape • Wrap the tape around the neck & fasten securely. • Allow about 2 fingers space to avoid direct pressure on the back of neck but the tape should NOT BE TOO LOOSE either. • Duoderm may be applied to both corners of the mouth to prevent raw edges which could cause ulcers.
After applying the tapes or ties, the following should be observed: Points to Note • Confirm the tube placement & marking of the ETT. • Cut the tube to around 2cm about the designated marking after the position is confirmed with CXR post-intubation to reduce dead space ventilation. This is particularly important during weaning.
Hyperoxygenate & perform endotracheal as well as oral pharyngeal suction. • Assess the symmetrical chest expansion & air entry. Note any pulmonary distress due to irritation after shifting the ETT. Evaluate the pulse oximetry. • CXR may be required if abnormalities are detected or when tube displacement is suspected. • Insert a bite block if required to maintain tube patency or prevent damage from giving rise to an air leak. Points to Note
Hudak C M, Gallo B M & Morton P G (ed) 2002 Critical Care Nursing: A Holistic Approach. 7th ed Philadelphia: Lippincott. • Lynn-McHale D J & Carlson K K (ed) 2001 AACN Procedure Manual for Critical Care. 4th ed Philadelphia: Lippincott. • Urden L D, Stacy K M & Lough M E 2002 Thelan’s Critical Care Nursing: Diagnosis and Management. 4th ed St Louis: Mosby. References