Download
1 / 21
220 likes | 359 Vues
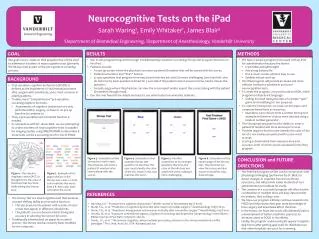
Neurocognitive Screening for POCD via the iPad. Sarah Waring and Emily Whitaker Advised by: Dr. James L. Blair, VUMC Anesthesiology Dept. Project Advisor. James L. Blair, OD Assistant Professor, VUMC Department of Anesthesiology

E N D
Neurocognitive Screening for POCD via the iPad Sarah Waring and Emily Whitaker Advised by: Dr. James L. Blair, VUMC Anesthesiology Dept.
Project Advisor • James L. Blair, OD • Assistant Professor, VUMC Department of Anesthesiology • Looking to develop pre-op screening for brain function using imaging and neurocognitive tests
Overview of POCD • Cognitive Dysfunction impairment of vital mental processes • After surgery with anesthesia post operative cognitive dysfunction (POCD) • Most common in elderly patients • Affects perception, memory, and information processing • Problems can persist for several months • Impedes activities of daily living (ADL)
Easy to read ink = word Trickier ink ≠ word Overview of Neurocognitive Tests • Stroop test • Assesses concept shifting ability and executive function • Name ink color, not the word • Example: http://www.cs.dartmouth.edu/farid/illusions/stroop.html
The Problem • “Comprehensive” pre-operative screening neglects brain • All other major organs are tested • Elderly patients often end up with some degree of POCD • Causes need for assistance with ADL • Causes increased mortality risk for next year
Current “Solutions” • Neurocognitive testing (NCT) after surgery to assess mental functions • One week and three months post-surgery • These tests determine presence of POCD • Accuracy without a pre-op baseline?
Group Purpose • A pre-operative test of mental function is needed • MRI/DTI/fMRI • Neurocognitive testing (NCT) • Values can be obtained for baseline • Physiological • Neurocognitive abilities • Can NCT be a screening tool for high risk of POCD? • Dr. Blair’s upcoming study will compare NCT results to physiological changes
Dr. Blair’s Hypothesis • 1. Serial MRI scans pre- & post-op will show anatomicchanges to structures associated with memory and executive function • 2. Compared to pre-op, there will be significant changes in functional neuroimaging • 3. NCT changes will correlate highly with alterations in functional and neuroanatomic substrates for memory and executive function as noted in 1 & 2
Group Objective • Create an iPad program that will be used to administer a battery of neurocognitive tests as part of the pre-op screening process • Must be: user friendly, in touch screen format, easy to administer, and take approx. 10 min. • Develop accurate scoring methods for program • Stroop test to start; other tests added later
How does our project fit in? • Dr. Blair’s study aims to determine if MRI can demonstrate changes in the central nervous system pre-op vs. post-op, and how these changes relate to neurocognitive tests given at the same time points • Our program will provide the data for the neurocognitive tests to compare to imaging data • Both sets of data will be used to determine if there is a correlation between CNS changes (both structural and functional) and anesthesia and surgery
How does our project fit in? • The iPad program will provide an easier and more efficient method to administer and score the neurocognitive testing portion of the study
Why an iPad? • More portable than a laptop • Lightweight • Don’t have to open/close • Longer battery life • Touch screen • Easy to use, especially for the elderly • Instant start-up
Completed Work • Met with Dr. Blair to discuss overall project objectives • Received project protocol • Decided to focus initially on Stroop test • Research into Stroop test, both paper- and computer-based versions • Research into POCD • Research into iPad programming
Current Work • Initial program coding • Research into relevant neurocognitive tests • Searching for computerized versions of Stroop test, “finger tapping,” JLO, and HVLT • Research into licensing of tests
Future Work • Continue to meet with Dr. Blair to discuss our role in project • Determine appropriate scoring method for Stroop test • Finish program coding • Begin testing • Administer to patients and test program performance
Long Term Implications • iPad format: • Combination of multiple tests into one program cuts costs • Easy transfer of data for analysis • Scoring algorithm: • Results calculated quickly • Data all in the same format • Trained proctor not necessary
Long Term Implications • Decrease number of cases of post-operative cognitive dysfunction • Decrease lawsuits associated with POCD • Gain more knowledge of POCD/how surgery and anesthesia affect the brain
What changes might occur if we have valid information? • Better understanding of relationship between cognitive and neurophysical changes due to anesthesia and surgery • Aid in creating rank-order of toxicity of anesthetic agents and • develop better anesthetic practices to decrease anesthetic risk in the elderly
Cost-Benefit Analysis • Costs • iPad • Our time – for production and coding • No actual $ costs associated with developing the program • Free to register as an Apple Developer • iOS Developer Program – needed to test application and distribute via App Store
Cost-Benefit Analysis • Benefits • Most important benefit – knowledge of anesthesia’s effect on the brain • Once tested, will be able to share with other hospitals to reduce POCD cases • Reduced lawsuits and legal fees • Potential for sale in the App Store
References • Hanning CD. Postoperative cognitive dysfunction. Br J of Anaesth. Jan 2005;95(1):82-87 • Monk TG, Weldon BC, Garvan CW, et al. Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology. Jan 2008;108(1):18-30 • Monk TG, Saini V, Weldon BC, Sigl JC. Anesthetic management and one-year mortality after noncardiac surgery. Anesth Analg. Jan 2005;100(1):4-10