Download
1 / 39
420 likes | 712 Vues
Diabetes and Heart Failure: A Comprehensive Collaboration. Grace Zite RN, MSN, CCRN, CCNS-Cincinnati Sarah Andrews RN, BSN-Lexington Keith Edinger RN, BSN-Pennsylvania Ashley Hancock RN , BSN-Houston Ed Park RN,CCRN, BSN-New Jersey Traceee Rose RN, BSN-San A ntonio.

E N D
Diabetes and Heart Failure: A Comprehensive Collaboration Grace Zite RN, MSN, CCRN, CCNS-Cincinnati Sarah Andrews RN, BSN-Lexington Keith Edinger RN, BSN-Pennsylvania Ashley Hancock RN, BSN-Houston Ed Park RN,CCRN, BSN-New Jersey Traceee Rose RN, BSN-San Antonio
Describe the disease process of Heart Failure (HF), and understand treatment regimens. • Describe the disease process of Diabetes Mellitus (DM), and understand treatment regimens. • Discuss the importance of educating pt.'s with HF and DM and provide tools to help with instructions to prevent negative outcomes. • Relate the impact of both disease processes on the quality of life and incorporate the synergy model to guide treatment. Objectives
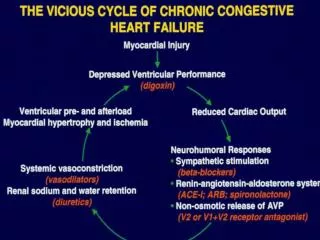
Impaired function/structure of one or both ventricles, producing inadequate cardiac output to meet the needs of tissues, and characterized by volume retention, congestion, and poor perfusion. Heart Failure
Coronary heart disease (CAD) and myocardial damage ( Acute myocardial infarction (AMI) is the cause in 75% of cases) • Chronic hypertension (HTN) ( 2nd most frequent cause). • Cardiomyopathy ( restrictive, dilated, or hypertrophic). • Mitral or aortic valve disease, septal defect, endocarditis. HF causes
Myocardial ischemia • Severe HTN • Dysrrthymias • Negative inotropic medications • Infection • Pulmonary embolism (PE) • Hyper/hypothyroidism • Diabetes Precipitating factors:
-Audible congestion - Ascites/ edema - Rales/ S.O.B. - Obtunation - JVD - Hepatic tenderness - Hypotension - Cool extremities - Narrow pulse pressure - Fatigue - Elevated BUN/ Creatinine Symptoms- HF
Pharmacological- *Diuretics * ACE inhibitors *Beta blockers * ASA * Statins * Vasodilators * Neurohormonal antagonists * Anticoagulants* *Antidysrrhtymics * Inotropes. Compliance with medication regimen per MD./ARNP. • Weight Control { includes daily weights to monitor fluid retention}. • Diet Modification- Cardiac diet {Low salt, low fat, fluid restriction} limit ETOH, Fresh foods- fruits & vegetables. • Exercise • Life-style modification Treatments- HF
DM is a disease where the body fails to properly produce or use insulin. Insulin is a hormone that turns sugar and other foods into another form or energy that can be used by the cells that make up the entire body. Other forms of DM exist ( gestational, medication induced, pre-diabetes), but, two major types are discussed clinically when the term “Diabetes” is mentioned: Type I DM – When the body can not produce insulin, which is a hormone that causes the cells to absorb glucose for fuel. About 5-10% of people have type I DM. Type II DM- When the body manages to produce insulin but fails to use it properly. Diabetes
Causes:Type I - 1.Family Hx. 2. Viral infections ( rubella, mumps). Usually Diagnosed in children and young adults. Type II- 1. Sedentary life-style. 2. Excess body weight. 3. HTN. 4. High cholesterol. 5. Family Hx . • Dx. : 1. Fasting blood sugar (BS). + if BS is >110 & < 126 mg/dL. 2. Oral glucose tolerance test (OTT). Pt. drinks glucola ( 75g of glucose or 100 g for pregnant pt.'s.) BS is checked at 30 min, 1 hr., 2hrs. & 3hrs post glucola ingestion. + if BS is > 140 or < 200mg/dL. *DM*
Type I: Type II: -Increased thirst & urination - Dry skin -Increased appetite - Skin Ulcers -Fatigue - Numbness of hands & feet -Blurred vision - Blurred vision -Frequent/slow healing infections - Dehydration - Wgt. Loss/gain Symptoms- DM
Pharmacological- *INSULIN- (fast, intermediate, basal insulin's) *Oral hypoglycemics ( metformin, actos, glyburide) *Blood pressure & *cholesterol lowering medications. • Dietary modification { high fiber, low saturated fats, carbohydrate modification. • Exercise • Weight control • Monitoring BS ( finger sticks, A1c monitoring). Treatment of Diabetes
Oral medication should be initiated when lifestyle changes do not control blood glucose levels (Pinhas-Hamiel & Zeitler, 2007) • Oral medications include: Biguanides, Thiazolidinediones, Sulfonylureas, Meglitinide analogs, and Glucosidase inhibitors (Pinhas-Hamiel & Zeitler, 2007) • Insulin therapy may be necessary for patients with uncontrolled blood glucose levels (Cirone, 1996) Pharmacology
Sulfonylurease are the most commonly prescribed hypoglycemic drugs in patients with heart failure • Retrospective cohort studies in the US involving more than 16,000 patients with DM and HF did not show link between sulfonylurea use and mortality • A Canadian retrospective cohort study compared Metformin to sulfonylurea use – one year mortality in patients treated with Metformin was lower than in patients treated with sulfolylureas • Consider use of a sulfonylurea if Metformin is contraindicated or when given in combination with metformin • (MacDonald, 2009) Pharmacology cont.
2 out of 3 fail to meet the goal of 6.5 % HG A1c set by: • American Diabetic Association • American Association of Clinical Endocrinologist • European Association of the Study of Clinical Diabetes Evaluating Glycemic Control Levich, B. R. ( 2011). Diabetes Management Optimizing Roles for Nurses in Insulin Initiation. Journal of Multidisciplinary Healthcare
Psychosocial barriers to glycemic control • Negative attitude toward insulin therapy initiation • Guilt by the HCP: failed medical management • Feeling like a failure with self management • Belief in restricted life style • Belief that insulin is the “last resort” • Fear of hypoglycemia ( Benroubi, 2011) The DAWN study Benroubi, M. (2011). “Fear, guilt feelings and misconceptions: Barriers to effective insulin treatment in type 2 diabetes” Diabetes Research and Clinical Practices. 97-99.
In the United States, 5 million individuals live with heart failure. • Two thirds of HF pt.'s. die within 5 years of being diagnosed. • The estimated annual cost in the United States is 56 billion annually. • Medicare spends more on HF than all forms of cancer. • HF hospitalizations have tripled over the last 25 years. • Most common reason for hospital admissions for pt.'s. > 65 yrs. • Greatest contributor to the cost of HF treatment is hospitalizations. • Affects Men > Women, but more women than men are admitted for HF. Statistics- Heart Failure
About 20.8 million children and adults in the United States or 7% of the population have DM. • 30% of adults in the United States have pre- diabetes….men > women. • 14.6 million have been Dx. with DM, but 6.2 million people are unaware they have DM. • Affects 10.6 % of all Hispanics & 10.8 % of all African Americans in the United States. • DM was the 7th leading cause of death in 2006 . • Most common cause of blindness, kidney failure, & amputations in adults & a leading cause of Heart disease & stroke. • African Americans are more likely to suffer from higher incidences of DM disabilities & complications. • DM is rare in youth ages 12-19 years, but about 16% have pre-diabetes. • One of the major risk factors for CAD leading to Heart Failure • 20-25% present in HF patients Statistics- Diabetes
Diabetic cardiomyopathy is defined as significantly impaired cardiac function in diabetic patients in the absence of epicardial vascular disease, left-ventricular hypertrophy, valvular disease, or other causes of cardiomyopathy, making it largely a diagnosis of exclusion. • The association between diabetic cardiomyopathy and diabetic retinopathy suggests that microvascular abnormalities may play a role. • One of the major risk factors for CAD leading to Heart Failure • 20-25% present in HF patients Diabetic Cardiomyopathy
Affects 180 million worldwide • 2/3 of patients with established CVD have impaired glucose • Affects 30% of HF patients • Every 1% increase in HgbA1c leads to an 8% increase in HF Diabetic Cardiomyopathy
High proisulin, hyperinsulinemia, hyperglycemia level Endothelium damage Accelerated atherosclerosis, cardiovascular remodeling Increased mortality Understanding DM Effect on HF
“apple a day keeps the doctor away”“Effective self care keeps hospital away” Goal of Self Care
optimize metabolic control • Hg A1c < 6.5% • prevent acute and chronic complications • Preventable hospitalization • Prevent Multi-organ dysfunction • optimize quality of life Goal of Self Care Carlson, Karen K. (Ed.) (2009). Advanced critical care nursing. (8th ed.) St. Louis, MO: Saunders
Know what you are teaching. • Medications • Keep updated with current guidelines and evidence-based practice • Avoid overwhelming the patient • Feel like drinking from a fire hose. • Is their “life” over? • Psychosocial • What is all this going to cost? Pearls of Patient Education
Pt’s. with HF & DM must struggle with necessary treatment regimen’s in order to maintain stability to achieve a sense or normalcy . • Increase in survival rates after acute Myocardial infarction (AMI) {due to newer medical advances}, aging population, and increased obesity rates will increase the rates for DM and HF complications. • Vulnerable groups ( elderly, & minorities) find themselves predominantly affected by theses diseases due to lack of resources, access to health care, and heredity. • Nonadherence to treatment regimens presents another challenge in treating DM/HF, which has many origins. Challenges
Pt. teaching/education. Not only is it important for the RN to educate the Pt. on DM & HF, but the RN must be confident in knowing the disease process so the right information can be distributed to enhance care. • Collaborate with members of the healthcare team to ensure the pt. is ready for discharge from the hospital. • Comply with core measures upon hospital discharge to reduce re-admission. • Provide resources and literature for DM/HF care upon discharge to help pt’s comply with treatment regimens Helping Pt.'s Face Challenges
Identify & correct precipitating causes of DM/HF. • Relieve symptoms, enhance comfort. • Enhance cardiac performance and control BS & decrease the progression of theses diseases. • Provide the tools & resources to keep pt.'s. compliant with their treatment regimens. • Decrease morbidity • Decrease hospitalizations • INCREASE THE QUALITY OF LIFE Goals & Purpose of Care
American Heart Association • www.heart.org • American Diabetes Association • www.diabetes.org • Center for Disease Control • www.cdc.gov • Heart Failure Society of America • www.hfsa.org • American Dietetic Association • www.eatright.org Patient Resources
The synergy model identifies 8 patient characteristics: resiliency, vulnerability, stability, complexity, resource availability, participation in care, participation in decision making, and predictability (Hardin & Kaplow, 2005) • 8 nursing competencies in the synergy model include: clinical judgment, advocacy, caring practices, collaboration, systems thinking, response to diversity, clinical inquiry and facilitation of learning (Hardin & Kaplow, 2005) • By using the synergy model, nurses will use their competencies to address the patient need that is presented (Hardin & Kaplow, 2005) Synergy Model
Stability: Frequency of dyspnea, weight gain and hospitalization • Complexity: Stage of HF, and co morbidities like DM, HTN, COPD, etc • Predictability: instabilities and other comorbities • Resiliency: Willingness to learn and follow self care regimen to regain equilibrium • Vulnerability: Consistency of social and financial support • Participation of Decision Making and Care: Cognitive capacity? Family member ? • Resource Availability: Family, community or governmental support ? Synergy Model Hardin, S., & Hussey, L. (2003). AACN Synergy Model for Patient Care: Case Study of a CHF Patient. Critical Care Nurse, 23,73-76. Retrieved from http://ccn.aacnjournals.org/content/23/1/73.full
Case Study Hardin, S., & Hussey, L. (2003). AACN Synergy Model for Patient Care: Case Study of a CHF Patient. Critical Care Nurse, 23,73-76. Retrieved from http://ccn.aacnjournals.org/content/23/1/73.full
Benroubi, M. (2011). “Fear, guilt feelings and misconceptions: Barriers to effective insulin treatment in type 2 diabetes” Diabetes Research and Clinical Practices. 97-99. Carlson, Karen K. (Ed.) (2009). Advanced critical care nursing. (8th ed.) St. Louis, MO: Saunders Funnell, M. M. (2006). The Diabetes Attitudes, Wishes, and Needs (DAWN) Study. Clinical Diabetes.(24) 154-155. Doi: 10.2337/diaclin.24.4.154 Hardin, S., & Hussey, L. (2003). AACN Synergy Model for Patient Care: Case Study of a CHF Patient. Critical Care Nurse, 23,73-76. Retrieved from http://ccn.aacnjournals.org/content/23/1/73.full Hunt, S., Baker, D., Chin, M., Cinquegrani, M., Feldman, A., Francis, G.,...Smith, S. (2001). Circulation. ACC/AHA Guilelines for Evaluation and Management of Chronic Heart Failure in the Adult: Executive Summary A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American Heart Association, 104: 2996-3007. doi: 10.1161/hc4901.102568 Lahm, T. , McCaslin, C. A., Wozniak, T.C., Ghumman, W., Fadl, Y.Y., Obeidat, O. S., Schwab, K., & Meldrum, D.R. ( 2010). Medical and Surgical Treatment of Acute Right Ventricular Failure. Journal of the American College of Cardiology Journal of the American College of Cardiology. 56, (18 ) 1435–46.doi:10.1016/j.jacc.2010.05.046 Lee, C. S., & Tkacs, N.C. (2008) Current Concepts of Neurohormonal Activation in Heart Failure. Mediators and Mechanisms. AACN Advanced Critical Care, 19 (4), 364–385. Retrieved from http://www.aacn.org/WD/CETests/Media/CI1942.pdf Levich, B. R. ( 2011). Diabetes Management Optimizing Roles for Nurses in Insulin Initiation. Journal of Multidisciplinary Healthcare. (4) 15-24 Stahl, M., & Richards, N. M. ( 2009). Update on Ventricular Assist Device Technology. AACN Advanced Care. 20, ( 1), 26-64. Retrieved from http://www.aacn.org/WD/CETests/Media/CI2012.pdf References
American Heart Association (2011). Understand your risk for heart failure. Retrieved from http:// www.heart.org/HEARTORG/Conditions/HeartFailure/UnderstandYourRiskforHeartFailure/Understand-Your- Risk-for-Heart-Failure_UCM • Debono, M., & Cachia, E. (2007). The impact of diabetes on psychological well being and quality of life. The role of patient education. Psychology, Health and Medicine, 12(5) 545-555. • Dries, D., Sweitzer, N., Drazner, M., Stevenson, L., & Gersh, B. (2001). Prognostic Impact of Diabetes in Patients With Heart Failure According to the Etiology of Left Ventricular Systolic Dysfunction Journal of the American College of Cardiology, 38(2) 421-8. • Eurich, D., Tsuyuki, R., Majumdar, S., McAlister, F., Lewanczuk, R., Shibata, M., & Johnson, J. (2009, February 9). Metformin treatment in diabetes and heart failure: when academic equipoise meets clinical inquiry. BioMed Central, 10(12). doi: 10.1186/1745-6215-10-12 • Hunt, S., Baker, D., Chin, M., Cinquegrani, M., Feldman, A., Francis, G.,...Smith, S. (2001). Circulation. ACC/AHA Guilelines for Evaluation and Management of Chronic Heart Failure in the Adult: Executive Summary A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American Heart Association, 104: 2996-3007. doi: 10.1161/hc4901.102568 • Jansen, J., Van Weert, J., De Groot, J., Van Dulmen, S., Heeren, T., & Bensing, J. (2010). Emotional and informational patient cues: The impact of nurses’ responses on recall [Entire issue]. Patient Education and Counseling, 79 218-224 doi: 10.1016/j.pec.2009.10.010 • MacDonald, M., Petrie, M., Fisher, M., & McMurray, J. (2009). Pharmacologic Management of Patients With Both Heart Failure and Diabetes [6]. Treatment: Pharmacology, 126-132. • Maru, S., Gibowski, L., Koch, G., Petri, H., Stender, M., White, A.,...Simpson, R. (2005). Antidiabetic Drugs and Heart Failure Risk in Patients With Type 2 Diabetes in the UK Primary Care Setting [Entire issue]. Diabetes Care, 28
Preis, S., Pencina, M., Hwang, S., D’Agostino, Savage, P., Levy, D., & Fox, C. (2009). Trends in Cardiovascular disease risk factors in individuals with and without diabetes in the framingham heart study. Circulation, 120(3), 212-220. Van Melle, J., Bot, M., De Jonge, P., De Boer, R., Van Veldhuisen, D., & Whooley, M. (2010). Diabetes, glycemic control, and new-onset heart failure in patients with stable coronary artery disease. Diabetes Care, 33(9), 2084-2089. National Institute of Diabetes and Digestive and kidney Disease (2009). New survey results show huge burden of diabetes. Retrieved from http://www.nih.gov/news/health/jan2009/niddk-26.htm National Diabetes Statistics, 2011 []. (2011). National Institute of Diabetes and Digestive and Kidney Diseases. Retrieved from www.diabetes.niddk.nih.gov Nesto, R., Bell, D., Bonow, R., Fonseca, V., Grundy, S., Horton, E.,...Kahn, R. (2003). A consensus statement from the American Heart Association and American Diabets Association [Consensus Statement]. . Oliver, S. (2010). The Role of the Clinical Nurse Specialist in the Assessment and Management of Biologic Therapies [Entire issue]. Musculosketal Care, 9 554-62 doi: 10.1002/msc.190 References