Download
1 / 48
490 likes | 724 Vues
Obesity Prevention in Early Childhood: Strategies for Healthy Development. Dianne S. Ward, EdD Department of Nutrition Gillings School of Global Public Health University of North Carolina at Chapel Hill. Outline. Introduction Childhood obesity as a health problem

E N D
Obesity Prevention in Early Childhood: Strategies for Healthy Development Dianne S. Ward, EdD Department of Nutrition Gillings School of Global Public Health University of North Carolina at Chapel Hill
Outline • Introduction • Childhood obesity as a health problem • Efforts to address childhood obesity prevention • Development of the NAP SACC program • Results from Pilot-testing of NAP SACC • Results from baseline studies of NAP SACC • Statewide evaluation of NAP SACC • Best practices for Healthy Weight Development at Child Care • NAP SACC dissemination • Next steps
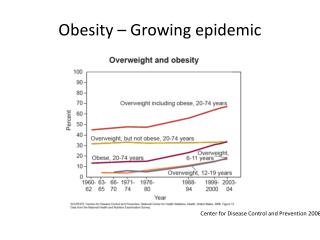
Childhood obesity is a serious public health problem in the US
21% of children ages 2-5 years are currently overweight or obese
The prevalence of childhood obesity is higher among ethnic minorities and children from low income families One of 7 low-income, preschool-aged children is obese, although trends may be slowing
Health Consequences Associated with Childhood Obesity • Increased risk of developing • Obesity in adulthood • Type 2 diabetes • Cardiovascular disease • Certain cancers
Childhood Obesity and Academic Performance Higher risk of micronutrient deficiencies e.g., iron, vitamin A Poor learning, cognition and school performance behavior problems Childhood obesity
Background • Poor dietary behaviors and physical inactivity increase risk for childhood obesity • 61% of US children ≤6 years are in child care • Foods and beverages consumed and physical activity in child care settings play a vital role in childhood obesity • Intervention efforts in child care settings can be effective for: • promoting healthful behaviors • ensuring children develop healthful food preferences early in life
Background • Limited childhood obesity prevention efforts target children <6 years old • More studies have focused on school-age children • Few interventions have focused on improving the nutrition and physical activity environments in childcare settings
Outline • Introduction • Childhood obesity as a health problem • Efforts to address childhood obesity prevention • Development of the NAP SACC program • Results from Pilot-testing of NAP SACC • Results from baseline studies of NAP SACC • Statewide evaluation of NAP SACC • Best practices for Healthy Weight Development at Child Care • NAP SACC dissemination • Next steps
The NAP SACC Program NutritionAndPhysical ActivitySelfAssessment for ChildCare
Intervention Development Interviews Focus groups Standards review Advisory group formation Pilot testing
NAP SACC Components Self-Assessment Action Planning Workshop Delivery Technical Assistance Evaluate, Revise, Repeat
Step 1: Self-Assessment • Facility director completes self-assessment instrument with help from key staff, such as the cook or program planner.
Step 2: Action Planning • Provider-generated with Consultant support • 3 Key Areas selected for improvement • At least 1 nutrition and 1 physical activity key area selected
Step 3: Workshop Delivery • 5 workshops (approved for 5.5 CEUs)
Step 4: Provision of Technical Assistance • This may be the most important step in the process!! • In-person, telephone, email • This offers... • Support • Encouragement • Additional information • A reminder of goals
Step 5: Reassessment • Evaluate • Centers complete follow-up self-assessment instrument to evaluate changes made during 6-month intervention • Revise • Repeat
Outline • Introduction • Childhood obesity as a health problem • Efforts to address childhood obesity prevention • Development of the NAP SACC program • Results from Pilot-testing of NAP SACC • Results from baseline studies of NAP SACC • Statewide evaluation of NAP SACC • Best practices for Healthy Weight Development at Child Care • NAP SACC dissemination • Next steps
Pilot-testing of NAP SACC • To assess feasibility and acceptability of NAP SACC • Randomized controlled trial • Convenience sample • n = 19 child care centers from 8 counties in NC (n=15 intervention centers; n = 4 comparison centers) • NAP SACC intervention was conducted over a 6-month period at intervention centers
Results from Pilot-testing of NAP SACC • Significant increase in self-assessment scores for nutrition, physical activity, and nutrition and physical activity combined after intervention • Feasibility and acceptability of NAP SACC • NAP SACC consultants • 80% agreed that self-assessment tool was comprehensive • 40% agreed, and 50% somewhat agreed that self-assessment was easy to understand • 70% agreed that meetings with center directors were productive • 60% agreed, and 40% somewhat agreed that they felt confident that they could deliver the NAP SACC program
Results from Pilot-testing of NAP SACC • Feasibility and acceptability of NAP SACC • Reports from Directors of child care centers • Self-assessment was fairly easy (36%) or very easy (64%) to use • Self-assessment was very helpful (83%) or somewhat helpful (17%) measure of the centers’ nutrition environments • Self-assessment was very helpful (50%) or somewhat helpful (50%) measure of centers’ physical activity environments • 12 said they would recommend NAP SACC to other centers • Changes in nutrition and physical activity policies and practices of their centers e.g., serving more fruits and vegetables
Outline • Introduction • Childhood obesity as a health problem • Efforts to address childhood obesity prevention • Development of the NAP SACC program • Results from Pilot-testing of NAP SACC • Results from baseline studies of NAP SACC • Statewide evaluation of NAP SACC • Best practices for Healthy Weight Development at Child Care • NAP SACC dissemination • Next steps
NAP SACC Baseline Studies: Diet • Baseline studies assessed nutrition practices and physical activity environments in child care centers • Study 1 • To determine whether foods consumed by children aged 2-5 years in child care centers meet their MyPyramid recommendation • Dietary observations were conducted in 1 classroom (n = 6 children) at each center • n = 117 children
Results from NAP SACC Baseline Studies • Summary of findings • Children consumed less than recommended amounts of • Whole grains • Fruits • Vegetables • Children consumed excessive amounts of • Added sugars from sweets and condiments • Saturated fat from whole milk and high-fat or fried meats
NAP SACC Baseline Studies: Physical Activity • Study 2 • To determine the association between the social and physical activity environment in child care centers • 1-day assessment using the Environment and Policy Assessment and Observation Instrument (EPAO) (n = 20 centers) • EPAO is an expanded version of the self-assessment instrument used in NAP SACC • Observed 4 children ages 3-5 year old at each center • Reviewed documents e.g., lesson plans, parent and staff handbooks
NAP SACC Baseline Studies: PA • Summary of findings • Centers with higher physical activity environment scores on the EPAO had children who • Were more physically active • Spent less time in sedentary activities • Had higher mean physical activity levels
Environmental factors associated with physical activity behaviors • Active opportunities (opportunities that result in MVPA) • Portable play equipment (e.g., jumping equipment, hula hoops, balls) • Fixed play equipment (e.g., climbing structure, running space, indoor play space) • Sedentary environment (e.g., television, computer, posters, books) • Physical activity training and education (e.g., PE curriculum, training for staff and parents)
Outline • Introduction • Childhood obesity as a health problem • Efforts to address childhood obesity prevention • Development of the NAP SACC program • Results from Pilot-testing of NAP SACC • Results from baseline studies of NAP SACC • Statewide evaluation of NAP SACC • Best practices for Healthy Weight Development at Child Care • NAP SACC dissemination • Next steps
Sample NAP SACC Evaluation Design • A convenience sample of 96 child care centers recruited from 33 North Carolina (NC) counties • Centers represented all three regions of NC (Western, Eastern, and Central Piedmont). • Most (n=84) were part of an evaluation of the NAP SACC intervention (Ward et al., AJPM, 2008); 12 additional centers were part of an exploratory study to test the self-assessment instrument.
Intention-to-Treat Model* • 56 intervention vs. 26 comparison centers (2 centers closed) • Intervention centers increased in both nutrition and physical activity areas, but only nutrition approached significance (p=.06) • When centers that did not start the intervention were eliminated (15), changes in the nutrition environment were significant (p<.01) *Does not include 2 centers that closed
Best Practice Guidelines for Nutrition 31 Best Practice Guidelines 8 key areas of the child care environment Fruits and Vegetables Meats, Fats, and Grains Beverages Feeding Practices Foods Outside of Meals and Snacks Supporting Healthy Eating Nutrition Education Nutrition Policies
Best Practice Guidelines for Physical Activity • Active opportunities • Fixed equipment • Portable equipment • Sedentary opportunities • Sedentary environment • Staff behavior • Training and education • PA policies • 25 Best Practice Guidelines • 8 key areas of the child care environment
Best Practices for Healthy Weight Development in Child Care • Conducted 2 studies to compare nutrition and physical activity in NC child care centers to best practice guidelines • n = 96 child care centers from 33 NC counties • Completed EPAO via one-day of observation in classrooms of 3-5y olds • Reviewed center documents e.g., menus, parent handbooks, staff training manual
Best Practices for Healthy Weight Development in Child Care • >50% of centers met best practice guideline to • Offer fried or pre-fried potatoes <1time/week or never • Make drinking water easily accessible to children • Locate soda/other vending machines off-site • Have staff encourage children to try new or less favored foods • Have staff join children and eat same foods during meals • Have formal nutrition policies that were followed
Best practices for Healthy Weight Development in Child Care • Areas for concern • <50% did not meet best practice guideline to • Offer fruit and vegetables ≥2 times/day • Offer high-fat meats <1 time/weekor never • Offer beans or lean meats >1 time/day • Offer 100% fruit juice <2times/week • Provide nutrition education opportunities for children and parents • 50% served whole milk instead of low fat fat milk
Best practices for Healthy Weight Development in Child Care • Most centers met best practice guidelines to provide • Teacher-led activities • Outdoor play • Outdoor play space and fixed play equipment • Portable play equipment • Ensure children are not seated for more than 30 minutes at a time • Areas for concern • Most centers did not provide at least 120 minutes of activity • 21% allowed children to watch >60 minutes of TV • At most centers, teachers did not join in active play • Most centers did not have formal written activity policies
Outline • Introduction • Childhood obesity as a health problem • Efforts to address childhood obesity prevention • Development of the NAP SACC program • Results from Pilot-testing of NAP SACC • Results from baseline studies of NAP SACC • Statewide evaluation of NAP SACC • Best practices for Healthy Weight Development at Child Care • NAP SACC dissemination • Next steps
States Using NAP SACC Intervention Materials NAP SACC Project
NAP SACC Program Identified as one of three model programs to address obesity prevention in child care. The other programs noted were Nemours Childhood Obesity Model, supported by the Nemours Health and Prevention Services and I am Moving, I am Learning, a health promotion and obesity prevention enhancement developed for Head Start.
National Resource Center forHealth and Safety in Child Careand Early Education NAP SACC was cited in Caring for our Children Guidelines National Resource Center for Health and Safety in Child Care and Early Education http://nrckids.org/CFOC/index.html
About 40% of the traffic on the CTRT site is seeking information about the NAP SACC program! http://center-trt.com/index.cfm
Next Steps Revise to include recommendations for infants and toddlers Modification of website to share barriers/promoters and success stories Possibility of adapting for family child care homes Possibility of linking child care healthy weight efforts to parents and home environment to promote healthy eating, regular physical activity, and healthy weight
Contact Us: Dianne Ward napsacc.org 919-843-0901 www.napsacc.org