Lynch Syndrome
Lynch Syndrome. Alicia Burillo, SPT Ithaca College 8/29/12 Memorial Sloan Kettering Cancer Center. Objectives . Define Lynch Syndrome Understand the role Lynch Syndrome plays in increasing risk factors for specific cancers Become familiar with screening and management of Lynch Syndrome

Lynch Syndrome
E N D
Presentation Transcript
Lynch Syndrome Alicia Burillo, SPT Ithaca College 8/29/12 Memorial Sloan Kettering Cancer Center
Objectives Define Lynch Syndrome Understand the role Lynch Syndrome plays in increasing risk factors for specific cancers Become familiar with screening and management of Lynch Syndrome Participate in a case study
What is Lynch Syndrome? Lynch Syndrome is a genetic disorder that predisposes individuals to developing certain cancers Also known as hereditary non-polyposis colorectal cancer syndrome (HNPCC) Mayo Clinic. Lynch Syndrome. Available at: http://www.mayoclinic.com/health/lynch-syndrome/DS00669/DSECTION=prevention. Accessed August 20, 2012.
History of Lynch Syndrome Named after Dr. Henry Lynch due to his work to characterize and emphasize importance of lynch syndrome HNPCC misleading name since disorder predisposes individuals to colon cancer as well as several other cancers Ahnen DJ, Axell L. Clinical features and diagnosis of lynch syndrome (hereditary nonpolyposis colorectal cancer). Up to date. 1-24.
Symptoms Colon cancer, or other cancers, that develop at a young age (before age 50) A family history of colon cancer that develops at a young age Family history of endometrial cancer Family history of related cancers, including ovarian, small bowel, stomach, urinary tract, pancreas, and hepatobiliary cancer Mayo Clinic. Lynch Syndrome. Available at: http://www.mayoclinic.com/health/lynch-syndrome/DS00669/DSECTION=prevention. Accessed August 20, 2012.
Lynch Syndrome Characteristics Autosomal dominant cancer syndrome accounting for 1-5% of colorectal cancers and 2% of endometrial cancers 50% chance for children to inherit genetic mutation for Lynch Syndrome from an affected parent Koornstra JJ, Mourits MJE, Sijmons RH, et al. Management of extracolonictumours in patients with Lynch Syndrome. Lancet Oncol 2009;10:400-408. Aarino M, Mecklin JP, Aaloten LA, et al. Life-time risk of different cancers in hereditary non-polyposis colorectal cancer (HNPCC) syndrome. Int. J. Cancer. Sept 1995;64:430-433.
Characteristics • Predisposesindividualsto develop: • Colorectal CA: 40-90%, • Endometrial CA: 27-71% • Ovarian CA: 6-24% • Stomach CA: 5-8% • Small bowel CA: 7% • Urinary tract CA: 4-12% • Pancreas CA: 4% • Hepatobiliary CA: 2% Aarino M, Mecklin JP, Aaloten LA, et al. Life-time risk of different cancers in hereditary non-polyposis colorectal cancer (HNPCC) syndrome. Int. J. Cancer. Sept 1995;64:430-433.
Characteristics Colon cancer, endometrial cancer or other related HNPCC cancers develop at an earlier age than cancers that develop sporadically without a family history Patients with LS who develop CRC have a 25-30% risk of developing a second primary CRC within 10 years of initial cancer Women with Lynch Syndrome have a 27-71% lifetime risk of developing endometrial CA compared to 3% for the general population Koornstra JJ, Mourits MJE, Sijmons RH, et al. Management of extracolonictumours in patients with Lynch Syndrome. Lancet Oncol 2009;10:400-408.
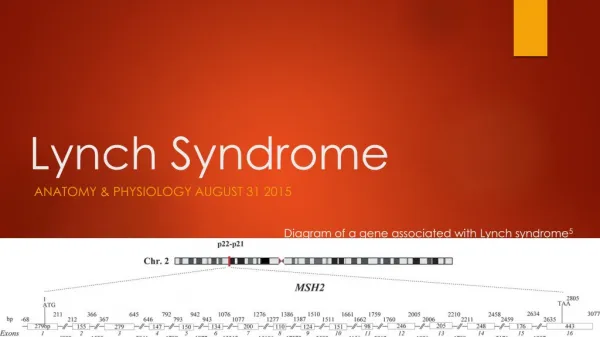
Causes • Germline mutations of specific genes that are involved in DNA mismatch repair. • MLH1 • MSH2 • PMS1 • PMS2 • The mutations lead to errors in replication of repetitive DNA segments, known as microsatellite instability (MSI). • The replication errors become widespread throughout the genome that trigger cancer development. Llor X. When should we suspect hereditary colorectal cancer syndrome?. Clinical Gastroenterology And Hepatology: The Official Clinical Practice Journal Of The American Gastroenterological Association. April 2012;10(4):363.
Diagnosis of Lynch Syndrome • Amsterdam II Criteria • There should be at least 3 relatives with a HNPCC associated CA (colorectal, endometrial, small bowel, ureter, or renal pelvis) • One should be a first degree relative of the other two • At least 2 successive generations should be affected • At least 1 relative should be diagnosed before age of 50 • Familial adenomatouspolyposis (FAP) should be excluded in the colorectal cases, if any. • Tumors should be verified by pathological examination Ahnen DJ, Axell L. Clinical features and diagnosis of lynch syndrome (hereditary nonpolyposis colorectal cancer). Up to date. 1-24. Llor X. When should we suspect hereditary colorectal cancer syndrome?. Clinical Gastroenterology And Hepatology: The Official Clinical Practice Journal Of The American Gastroenterological Association. April 2012;10(4):363.
Diagnosis of Lynch Syndrome • Revised Bethesda Guidelines for testing colorectal tumors for microsatellite instability (MSI) • Tumors should be tested for MSI in the following situations: • Colorectal cancer diagnosed in a pt < 50 yo • Presence of synchronous, metachronous colorectal, or other HNPCC related tumors, regardless of age • Colorectal cancer with the MSI-H histology diagnosed in a patient who is less than 60 years of age • Colorectal cancer diagnosed in a patient with one or more first-degree relatives with an HNPCC-related tumor, with one of the tumors being diagnosed under age 50 • Colorectal cancer diagnosed in a patient with two or more first or second degree relatives with HNPCC-related tumors, regardless of age. Ahnen DJ, Axell L. Clinical features and diagnosis of lynch syndrome (hereditary nonpolyposis colorectal cancer). Up to date. 1-24.
Diagnosis of Lynch Syndrome If Amsterdam or Bethesda criteria are met patients should undergo MSI analysis and/or immunohistochemistry (IHC) testing for MMR protein expression in tumor tissue. Patients with microsatellite unstable tumors should then be tested for MMR gene mutations Once a mutation is identified, family members can be tested for specific MMR mutation identified in family member Llor X. When should we suspect hereditary colorectal cancer syndrome?. Clinical Gastroenterology And Hepatology: The Official Clinical Practice Journal Of The American Gastroenterological Association. April 2012;10(4):363.
Screening for Lynch Syndrome Colonoscopies starting at 20-25 years of age or 2-5 years before earliest dx of CRC in family if diagnosed before age 25, repeat every 1-2 years Transvaginal US and endometrial biopsy yearly starting at 30-35 years of age for endometrial and ovarian cancer Women with LS associated endometrial CA should undergo screening for colorectal cancer due to high lifetime risk of developing a second primary malignancy. Prophylactic TAH/BSO for women no longer seeking fertility Llor X. When should we suspect hereditary colorectal cancer syndrome?. Clinical Gastroenterology And Hepatology: The Official Clinical Practice Journal Of The American Gastroenterological Association. April 2012;10(4):363. Meyer L, Broaddus R, Lu K. Endometrial cancer and Lynch syndrome: clinical and pathologic considerations. Cancer Control: Journal Of The Moffitt Cancer Center. January 2009;16(1):14-22. Auranen A, Joutsiniemi T. A systematic review of gynecological cancer surveillance in women belonging to hereditary nonpolyposis colorectal cancer (Lynch syndrome) families. ActaObstetricia Et GynecologicaScandinavica. May 2011;90(5):437-444.
Treatment Dependent upon type, stage, and location of cancer as well as prior health status. Treatment for colon cancer typically includes colectomy, chemotherapy, or radiation. Treatment for endometrial cancer typically includes TAH/BSO, chemotherapy, and radiation.
Prognosis Non-specific Dependent upon development and treatment of cancers (how many primary tumors, location of tumors, stage at diagnosis, success treatment options for cancer, etc.) No data to suggest the prognosis for women with LS associated endometrial CA is any different than for women with sporadic endometrial cancer. Meyer L, Broaddus R, Lu K. Endometrial cancer and Lynch syndrome: clinical and pathologic considerations. Cancer Control: Journal Of The Moffitt Cancer Center. January 2009;16(1):14-22.
Case Study • History: • 65 yo Female with Lynch Syndrome dx with stage I Endometrial CA in 2008 • Treated with TAH/BSO at OSH • Presented with R hip pain 5/2011 • Via x-ray found to have large pelvic mass encompassing R pelvic side wall and R iliac bone (Metastatic Adenocarcinoma) as well as hip fracture • Underwent chemo and radiation without success and continued pain • Admitted 4/23/12 and underwent R internal hemipelvic resection and THA with bladder involvement, ureter repair, and stent placement. Sciatic and internal iliac veins were cut. • Course c/b bladder leak, tissue necrosis, & fluid collection requiring wound vac placement and 5 rounds of irrigation and drainage • R nephrostomy placement on 6/11/12 • 6/27/12 R external hemipelvectomy • L nephrostomy placement on 7/27/12
Case Study • Re-eval following external hemipelvectomy • Presented with: IV, mediport, Foley catheter, 1.5L 02 via NC, PCA, JP, R nehprostomy bag • Cognition: A & O x3 • LLE WBAT • Diminished light touch to R residual limb and phantom limb sensations • Functional training: Rolling: Min –Mod A x2 • Co-treat with OT • Treatment/ rehab issues: • 5x/wk • rolling, supine sit, weight shift, sit stand, standing tolerance, bed chair • Complicated by severe anxiety & apprehension of pain Guo Y, Fu J, Palmer J, Hanohano J, Cote C, Bruera E. Comparison of postoperative rehabilitation in cancer patients undergoing internal and external hemipelvectomy. Archives Of Physical Medicine And Rehabilitation. April 2011;92(4):620-625.
Case Study • D/C plan • Acute rehab • According to study by Guo et al, acute rehab admission criteria include: • Inability to function I in ADL’s and/or mobility, neurogenic bowel/bladder, cognitive deficit, incoordination, dysarthria, spasticity, and the need for at least 2 of the following: PT, OT, Speech, or nursing. • According to this study inpatient rehab admission associated with older age: average age 55yo • Outcome measures: FIM or Barthel Index: valid and reliable tools to measure disability: help to determine realistic goals for pts
Case Study • Now: • Presents with: IV, PCA, drains, B nephrostomy bags • Cognition: A & O x3 • Diminished light touch to R residual limb and phantom limb sensations • Level 1 therapeutic exercise • Functional training: • Rolling with S • Scooting Min A x1 • Bridging Mod I with trapeze • Supine sit S • Sit stand with RW Min A x2, • Stand sit with CG • Bed chair Min A x2 • Perform 1 hop backward • Can tolerate sitting 45 min in w/c • PT works with rehab assistant • Demonstrates decreased anxiety and apprehension • Went from 4x/wk back to 5x/wk • D/C recsubacute rehab
Literature • Title: External hemipelvectomy as treatment for solitary coxofemoral metastasis from endometrial carcinoma: Case report and review of the literature • Presentation: 62yo female with increasing L hip pain developed bone met from endometrial CA • Treatment: • Chemo with no clinical response • External hemipelvectomy with TAH/BSO • Outcome measures taken before, 3 & 6 months later: • Barthel index • LASA (Linear Analog Scale Assessment) • Showed decreased ability to perform ADL’s • Barthel prior: 100, 6mos after: 70 • no change in QOL • LASA QOL score prior: 77, 6mos after: 70 • Still alive at 6 months, unsure of overall survival time Vizzielli G, Fanfani F, Costantini B, Gallotta V, Scambia G, Fagotti A. External hemipelvectomy as treatment for solitary coxofemoral metastasis from endometrial carcinoma: case report and review of the literature. The Journal Of Obstetrics And Gynaecology Research. May 2012;38(5):892-898.
References Mayo Clinic. Lynch Syndrome. Available at: http://www.mayoclinic.com/health/lynch-syndrome/DS00669/DSECTION=prevention. Accessed August 20, 2012. Ahnen DJ, Axell L. Clinical features and diagnosis of lynch syndrome (hereditary nonpolyposis colorectal cancer). Up to date. 1-24. Koornstra JJ, Mourits MJE, Sijmons RH, et al. Management of extracolonictumours in patients with Lynch Syndrome. Lancet Oncol 2009;10:400-408. Aarino M, Mecklin JP, Aaloten LA, et al. Life-time risk of different cancers in hereditary non-polyposis colorectal cancer (HNPCC) syndrome. Int. J. Cancer. Sept 1995;64:430-433. Llor X. When should we suspect hereditary colorectal cancer syndrome?. Clinical Gastroenterology And Hepatology: The Official Clinical Practice Journal Of The American Gastroenterological Association. April 2012;10(4):363. Meyer L, Broaddus R, Lu K. Endometrial cancer and Lynch syndrome: clinical and pathologic considerations. Cancer Control: Journal Of The Moffitt Cancer Center. January 2009;16(1):14-22. Auranen A, Joutsiniemi T. A systematic review of gynecological cancer surveillance in women belonging to hereditary nonpolyposis colorectal cancer (Lynch syndrome) families. ActaObstetricia Et GynecologicaScandinavica. May 2011;90(5):437-444. Guo Y, Fu J, Palmer J, Hanohano J, Cote C, Bruera E. Comparison of postoperative rehabilitation in cancer patients undergoing internal and external hemipelvectomy. Archives Of Physical Medicine And Rehabilitation. April 2011;92(4):620-625. Vizzielli G, Fanfani F, Costantini B, Gallotta V, Scambia G, Fagotti A. External hemipelvectomy as treatment for solitary coxofemoral metastasis from endometrial carcinoma: case report and review of the literature. The Journal Of Obstetrics And Gynaecology Research. May 2012;38(5):892-898.