Download
1 / 43
490 likes | 1.48k Vues
Treatment of Ankylosing Spondylitis. Enbrel RA MENA Speaker Bureau Dubai, United Arab Emirates January 2009 Prof. Joachim R. Kalden Director emeritus Medical Department III Div. for Molecular Immunology University of Erlangen-Nuremberg. Ankylosing Spondylitis Overview.

E N D
Treatment of Ankylosing Spondylitis Enbrel RA MENA Speaker Bureau Dubai, United Arab Emirates January 2009 Prof. Joachim R. Kalden Director emeritus Medical Department III Div. for Molecular Immunology University of Erlangen-Nuremberg
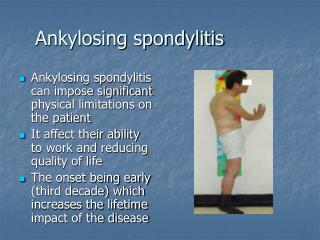
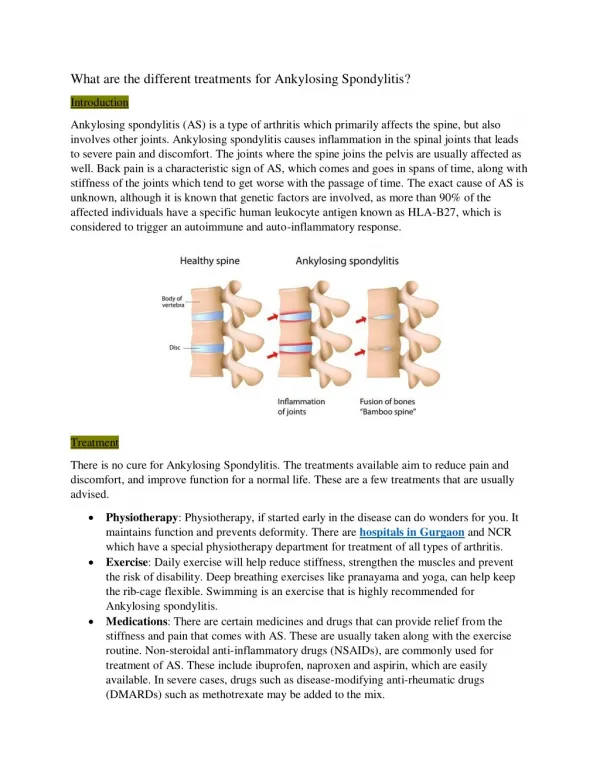
Ankylosing Spondylitis Overview • A type of arthritis that causes inflammation and eventually fusion of the spine and the spinal joints. Involvement of peripheral joints and extraarticular manifestations. • AS causes pain, stiffness, disability, decreased spinal mobility, and decreased quality of life • The prevalence ranges from 0.1 to 1 percent of the population • Men are affected three times more than women • Commonly develops between the ages of 15 and 40 • 95 percent of people with AS share the genetic marker HLA-B27
Treatment of Ankylosing SpondylitisOverview • Treatment goals • Use of traditional therapies • Clinical results with TNFalpha antagonists • Guidelines for the management of TNFalpha antagonists
Treatment goals in Ankylosing Spondylitis • Reduce and or prevent deleterious effects of: • Inflammation • Ankylosis • Abnormal posture Inhibition of osteoblastogenesis Dougados et al. J.Rheumatol 2001;28-62:16-20.
Development of Ankylosis in Ankylosing Spondylitis • The earliest change seen was a sub acute osteitis in the immediately adjacent bone. • This was followed by extensive replacement of the fibrocartilage and adjacent bone by fibrous tissue in which there was often little remaining evidence of inflammation. • The late stage of the disease in this joint consisted of assification. From: Cruickshank and Path, Pathology of Ankylosing Spondylitis
bone marrow bone Late Stage Reparation Mechanism - Dense Formation of Osteoblasts Appel H, Loddenkemper C, Sieper J; unpublished
ASAS/EULAR Recommendations for the Management of AS Education, exercise, physical therapy, rehabilitation, patient associations, self help groups NSAIDs Ana l ges i cs Axial disease Peripheral disease Su r ge r y Sulfasalazine Local corticosteroids TNF blockers Zochling J, et al. Ann Rheum Dis. 2006;65:442-52 (excerpt)
Celecoxib Versus Naproxen in AS:Improvements in Primary Efficacy Measures Barkhuizen et al. Ann Rheum Dis 2005;64(supplementIII);338(Abs).
Reduction of Radiographic Progression by NSAIDs in Ankylosing Spondylitis Inhibition of proliferation and migration of osteoblasts in a rat bone healing model by diclofenac GD Krischak et al. Arch Orthop Traum Surg 2007, 127:453-458 Wanders et al. Arthritis Rheum 2005;52:1756-65.
% patients placebo Sulphasalazine 59 60 43 42 40 40 20 Clegg et al. Arthritis Rheum 1999;42:2325-9. Periphral n=187 Axial n=187 Sulphasalazine in the Treatment of Spondylarthropathy Dougados et al. Arthritis Rheum 2005;38:618-27.
Conventional DMARDs in the Treatment of Ankylosing Spondylitis Sulfasalazine* 2 g/day Leflunomide** 20 mg/day Methotrexate† 20 mg/week sc 8 8 8 7 6 6 6 5 P=0.03 BASDAI (mean) 4 4 4 BASDAI (mean) BASDAI (mean) 3 2 2 2 All patients (n=20) Peripheral arthritis (n=10) Placebo (n=60) 1 All patients (n=20) Sulfasalzine (n=60) Non-arthritis (n=10) 0 0 0 0 4 8 12 16 20 24 0 4 8 12 16 20 24 0 4 8 12 16 Week Week Week *Braun J, …, Sieper Jl. Ann Rheum Dis 2006 Apr 10; Epub **Haibel H, ..., Sieper J. Ann Rheum Dis2005;64:124-6. †Haibel H, .... Sieper J. 2006; Aug 10; Epub.
Conclusions from treatment experiences in Ankylosing Spondylitis with traditional therapies • Traditional therapy options are not sufficient to treat active disease • Physiotherapy important to maintain function • NSAIDs alleviate pain in some but not all patients • Steroids and immunomodulators have little/no effect • No drugs which impede disease progression • Unmet medical need in the treatment of severe AS
Infliximab Monotherapy Study In Active Ankylosing Spondylitis Study Design Open Label Double-Blind Baseline Period Loading Period Placebo (N=35) Infliximab 5mg/kg Q 6 Wks 70 Patients Infliximab 5 mg/kg Q 6 Wks (N=35) Infliximab 5 mg/kg Q 6 Wks 12 54 0,2,6 Week Braun et al. Lancet 2002;359:1187-93.
Percentage of Patients With Improvement of 50% in BASDAI 100 80 P<0.001 P<0.001 60 Placebo Patients responding, % P<0.001 Infliximab 5 mg / kg 40 20 0 0 2 4 6 8 10 12 Weeks Reduction of Disease Activity Was Rapid and Durable Through 12 Weeks Intent-to-Treat Population Braun et al. Lancet 2002;359:1187-93.
BASDAI 50% ASAS 40% ASAS 20% 5 out of 6 Maintenance of Efficacy of Infliximab in Ankylosing Spondylitis. Two year extension of a 3 months RCT Braun et al. Ann. Rheum Dis 2005;64:229-34.
Control group Control group Progression in total group Progression in group with damage at baseline Radiographic Progression in Patients with Ankylosing Spondylitis treated for 2 years with Infliximab Baraliakos et al. Ann Rheum Dis 2005;64:1462-6.
Anti-TNF therapy in AS: Continuous improvement of spinal mobility and function over 2 years Placebo-patientsCrossed-over Placebo-patientsCrossed-over 2 24 54 102 54 24 102 Braun J, et al. Arthritis Rheum 2008, in press
A randomized controlled clinical trial of infliximab shows clinical and MRI efficacy in patients with pos. HLA B27 and very early AS • 49 pat. with early inflammatory back pain, HLA B27 pos. and known oedema on MRI were randomized • No demographic changes between the two groups Result • Infliximab appears to be an effective therapy in very early inflammatory back pain (significant change from baseline: MRI score of sacroiliac joints resolving of SI-joint lesions. Improvement of clinical parameters) N. Barkham et al. ACR 2007. L11
100 75 58 51 50 41 39 25 21 19 14 14 Adalimumab in Ankylosing Spondylitis. The ATLAS trial: a RPCT on 315 patients treated for 24 weeks % patients placebo Adalimumab 40 mg eow ASAS 20 ASAS 40 ASAS 20 ASAS 40 12 weeks 24 weeks Davis et al. Arthritis Rheum 2005;S208 (abs.483).
Adalimumab in Ankylosing Spondylitis. The ATLAS Trial: a RPCT on 315 patients Treated for 24 weeks % patients 100 placebo Adalimumab 40 mg eow 75 50 22 21 25 6 4 Remission 12 weeks 24 weeks Davis et al. Arthritis Rheum 2005;S208 (abs.483).
Adalimumab in patients with total spine ankylosis • Randomized, placebo-controlled trial (ratio 2:1) • In patients with TSA adalimumab treatment resulted in rapid and clinically significant improvement in signs and symptoms of active disease • At week 12: 50% of adalimumab treated patients achieved ASAS 20, 33% ASAS 40, ASAS 5/6 and BASDAI 50 as compared to non of placebo treated patients • After 1 year: 8/11 adalimumab treated patients achieved ASAS 20 • After 2 years: 6/11 adalimumab treated patients achieved ASAS10 van der Heijde D et al, Ann Rheum Dis, Dec 2007
Etanercept for Ankylosing Spondylitis. Results of a 24-weeks RPCT on 277 patients Davis et al. Arthritis Rheum 2003;48:3230-6.
Sustained Durability of Etanercept in Ankylosing Spondylitis for 96 weeks Davis et al. Ann Rheum Dis 2006;64:1557-62.
Longterm anti-TNF therapy in AS - persistent low disease activity over 4 years BASDAI (0–100) 70 60 50 Mean BASDAI 40 RCT 30 20 *Week 24 represents the baseline of the OLE as well as the point of initial etanercept treatment for the patients switched from placebo to etanercept. Etanercept/Etanercept 10 Placebo/Etanercept 0 0 24* 48 72 96 120 144 168 192 Weeks Davis J et al. Ann Rheum Dis 2008
Long-term anti-TNF therapy in AS - continuous improvement of function BASFI (0–100) 60 50 40 Mean BASFI 30 20 *Week 24 represents the baseline of the OLE as well as the point of initial etanercept treatment for the patients switched from placebo to etanercept. Etanercept/Etanercept 10 Placebo/Etanercept 0 0 24* 48 72 96 120 144 168 192 Weeks Davis J et al. Ann Rheum Dis 2008
Assessment of Clinical Efficacy in a Randomized Double-Blind Study of Etanercept and Sulfasalazine in Patients With Ankylosing Spondylitis October 27, 2008 American College of Rheumatology Annual Scientific MeetingACR 2008 J. Braun,1 F. Huang,2 R. Burgos-Vargas,3 I.E. van der Horst-Bruinsma,4B. Freundlich,5 B. Vlahos,5 A.S. Koenig5 1RuhrUniversity, Bochum, Germany; 2ChinesePLA General Hospital, Beijing China; 3Hospital General de México and Universidad Nacional Autónoma de México, Mexico City, Mexico; 4VU University Medical Center, Department of Rheumatology, Amsterdam, Netherlands; 5Wyeth Research, Collegeville, PA, USA
Objective To compare the efficacy and safety of etanercept 50 mg once weekly with sulfasalazine 1.5 to 3 g daily over 16 weeks in patients with active ankylosing spondylitis (AS)1 1van der Linden S. et al. Arthritis Rheum 1984;27:361–8.
Key Endpoints • Primary • Proportion of patients achieving ASAS 20 (20% improvement by Assessment of AS criteria) at 16 weeks • Select Secondary • ASAS 20, ASAS 40, ASAS 5/6, partial remission1 • BASMI (Bath Ankylosing Spondylitis Metrology Index) • BASFI (Bath Ankylosing Spondylitis Functional Index) • BASDAI (Bath Ankylosing Spondylitis Disease Activity Index) • C-Reactive Protein through 16 weeks • Back pain • Modified Schober’s test 1Anderson et al. Arthritis Rheum 2001; 441876-86
Proportion of Patients Who Achieved ASAS 20 (LOCF) Primary Endpoint: Proportion of Patients Who Achieved ASAS 20 at week 16 * * * * * *P<0.001, etanercept versus sulfasalazine
Proportion of Patients Who Achieved Partial Remission* (LOCF) † † † † † *Anderson et al. Arthritis Rheum 2001; 441876-86; †P<0.001, etanercept versus sulfasalazine
Mean BASMI Scores (LOCF) * * * * * *P<0.001, etanercept versus sulfasalazine
Conclusions • In this 16-week study • Etanercept therapy was superior to sulfasalazine therapy in the treatment of subjects with ankylosing spondylitis. • There were no unexpected safety findings
Etanercept Shows Persistent clinical Efficacy over 5 Years According to: Baraliakos X et al., FRI0291, EULAR 2008 • At 5 Years (n = 18): • 33% were in partial remission according to ASAS criteria • 38% achieved a BASDAI 50% response • 62% achieved a ASAS 40% response • 65% achieved a ‘5 out of 6’ response
Effectiveness of Adalimumab after failure of infliximab or etanercept in patients with PsA and AS • Open-label phase IIb studies • PsA „STEREO“ 66 of 442 patients discontinued and were switched to adalimumab • AS „RAPSODY“ 309 of 1186 patients discontinued and were switched to adalimumab • PsA: Significant improvement in ACR 20, 50, 70 and HAQ • AS: Significant improvement in ASAS 20, 50, 70 and BASDAI Burmester et al. Arthritis Rheum 2007; 56, 393
Prediction of Response to TNF Antagonists in Ankylosing Spondylitis: Infliximab n=69, Etanercept n=30 <10, 11-20 years, >20 years <4.5, 4.5-6.5, >6.5 Rudwaleit et al. Ann Rheum Dis 2004;63:665-70.
Median percentage changefrom baseline Interferon-γ Interleukin-6 VEGF CRP Visvanathan Set al., Ann Rheum Dis, 2008
Better Response if AS Patients Treated Early in the Disease Course (n=100)(as judged by BASDAI 50 response) 80 73 58 60 % 40 31 20 0 <10 years, N=37 11-20 years, N=33 >20 years, N=29 Patients with Ankylosing Spondylitis (n=99) treated with TNFa-Blockers Rudwaleit M, et al. Ann Rheum Dis. 2004; 63:665-70
Discontinuation of anti-TNF Therapy in Ankylosing Spondylitis Baraliakos X et al., Arthritis Res Ther, 2005
Effects of TNFalpha antagonists on extra-articular manifestations Reduction in the number of enthesetic regions • Infliximab • Etanercept • Adalimumab Decreased incidence of anterior uveiitis • Infliximab • Adalimumab • Etanercept less effective Braun et al., Lancet 2002; 359:1187-93 Marzo-Ortego et al., Arthritis Rheum 2001; 44:2112-17 Braun et al., Arthritis Rheum 2005; 52:2447-51 Lyndell LL et al, Arthritis & Rheumatism (2007)56:3248-3252
Proportion of Patients with Enthesopathy The Impact Study Placebo cross-over to Infliximab 40 0 0 * p = 0.03 30 10 Phase II: All Patients Receive Infliximab; Original Blind Maintained Percent of Patients 20 * 10 0 0 16 50 16 50 0 Weeks C. Antoni et al. Arth Rheum 2003
International ASAS Consensus Statement for the Use of anti-TNF in Patients with Ankylosing Spondylitis • Indication Definitive AS • Active disease - BASDAI ≥4 • - expert opinion • - acute phase response • - imaging modalities • Failure of ≥2 NSAIDs • In case of peripheral arthritis failure of intraarticular • corticosteroids/sulphasalazine • Absence of contraindication • Monitoring BASDAI • ASAS core set • Responder: improvement of ≥2 units on BASDAI Baeten et al. Ann Rheum Dis 2003;62:829-34..
News from the ACR Meeting 2008 • Long-term efficacy for up to 7 years for all 3 TNF antagonists being licenzed for the treatment of AS. No new safety signals • Re-Treatment of AS patients who flaired after ADA treatment was stopped is possible • Early effective treatment of AS (as shown for ADA) might significantly improve the work productivity
Summary • TNF antagonists proven in PsA, AS to have a long-term clinical efficacy and acceptable safety profile • No new side effects reported in long-term clinical trials as compared to previous studies and registry data • Identical recommendation for screening patients before TNFalpha antagonist should be started • Psoriasis induced by TNFalpha antagonists • (Sfakis PP et al. Arthritis Rheum 2005) • (Kary S. Ann Rheum Dis 2006;65:405-407) • (Massara A et al. Rheumatology 2006;45:730-733)