Download
1 / 68
680 likes | 825 Vues
PHLEBOTHROMBOSIS. MUDr. Monika Laššánová. THROMBOSIS. = INTRAVITAL COAGULATION OF BLOOD IN VESSELS OR HEART Incidence of venosus thromboembolism – 0,1% 0,01% among persons cca. 20 years old 1,0% among persons cca. 60 years old.

E N D
PHLEBOTHROMBOSIS MUDr. Monika Laššánová
THROMBOSIS = INTRAVITAL COAGULATION OF BLOOD IN VESSELS OR HEART • Incidenceofvenosusthromboembolism– 0,1% • 0,01% amongpersons cca. 20 yearsold • 1,0% amongpersons cca. 60 yearsold
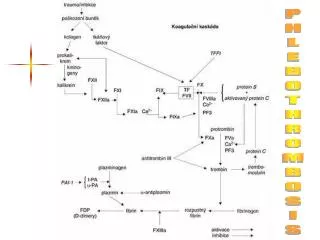
Patogenesisoftrombosis=(1856) – Wirchow´strias activation of COAGULATION = activity TXA2, activity anticoagulant sys. (AT III), levels or activation of coagulation f. ... slowing down of BLOOD FLOW = stasis, travelling with airplain, right heart failure, paraplegia, immobilisation, gravidity, varixes, operations, fractures ... deffect of VESSEL WALL – by damage of endothel production PGI2 => proaggregatory activity = neo, infusions, operations... Most important factors
Arterial trombi = white • Trombocytes • Tight adherence => obturation = periferal ischemia • Prevention = antiaggregants • Venal trombi = red • Fibrinal tail • No adherence => migrates = embolisation • Prevention and treatment = anticoagulants • Recent trombi • Are removed (trombolysis) = fibrinolytics
Clinicalconditionscausingthrombosis arterial: • atherosclerosis • smoking • hypertension • diabetes mellitus • LDL • TAG • possitive family history • deffect of left • oestrogens • polyglobulia … venosus: • general surgery • orthopedical surgery • trauma, malignities, sepsa • immobilisation • congesstive deffects • nefrotic syndrome • obesity • varixes • postphlebitic syndrome • oestrogens • gravidity
Different! thrombophlebitis phlebothrombosis
THROMBOPHLEBITIS • primarily with mechanic, microbial or chemical irritation inflammation of vessel wallsecondarily can occur thrombosis – forming of grey thrombus with many fibroblasts firmly adhering to vessel wall, connective tissue is organising embolisation occaisionally • clinically:local syndrome = inflammated firm superficial vein can be palpated, skin above is red, warm, significant pain and sensitivity, no oedema, no general signs or only subfebrility • complications: early – spreading of inflammation to deep venosus sys., late – sec. chronic venosus disease = postphlebitic syndrome
DeepVenosusThrombosis= Phlebothrombosis + its most dangerous complication = pulmonary embolus (PE) – belongs after ICHD and hypertension among the most often KVS diseases of hospitalised persons • PE - 10% of autopsial material • 85% is caused PE by deep venosus thrombosis
PHLEBOTHROMBOSIS (PT) • deep veins of lower extremities • primarily develops obturation of vein with thrombus and only secondarily develops small inflammatory reaction • released thrombus = embolus • clinically: often asymptomatic – or little symptoms = dg. only 30-50% • oedema – is assymetric = difference more than 2 cm • pain – spontanneous, at palpation, compressive – mainly at hanging down the limb, idle spasms, feeling of strain • erythematic - pale - cyanotic – symptom of block of blood flow from the limb • formed collaterals – as compensatory mechanism, after several days of obturation • systemic symptoms – a little specific
Clinicalsymptoms Lowerlimb: • pain • oedema( 1,5 cm) • posit. palp. manoeuvre(Homans, Lőwenberg,...) • enlargedsuperficialcollaterals • changeof skin collour and temperature
Complicationsof PT • EMBOLUS is by blood flow carried reliesed trombus – mainly to pulmonary artery pulmonary embolism • Repeated embolisation (successive) =>chronic pulmonary hypertension => cor pulmonale chronicum • Chronic venous insufficiency
Goalofthetreatmentof PT • acute condition • save patient´s life • inicialise and speed-up thrombembolic resolution • accelerate symptom regression • prevention of recurrency • reduce mortality
nonpharmacologic limb elevation (15-20º) soonmobilisationaftersurgery regularexcercisewithlegs in bed elastic, specialtights walking pharmacologic lowdosesofheparin(5000 IU) (beforeoperation, duringpostoperationperiodat risk patients) Preventionof PT
Situation:You are a generalpractitioner. Followingpatientcomes to you:
Mr. Novák iscomplaining, that , sinceplasterwasputdownfromhisright leg beforeoneweek, successivelyhisright leg gotswollen, hefeelspainatwalking and last 2 daysstartedwithdifficulty to breath. Hefeelsstitching on therightsideofchestgetting more emphasizedatinspiration. • Atphysicalexaminationobservedtachypnoe, accentationof 2nd heartsoundabovepulmonaryartery, attenuatedbreathingatbasalrightside, right leg swollenassymetrically, positiveHomans and Löwenberg. • Atlaboratoryexaminationhypoxia in arterialblood. • Workoutpharmacotherapeuticplan.
Antithrombotics • antiaggregants(antiplateletdrugs) = blockFORMATIONofthrombus • anticoagulants= blockGROWTH ofthrombus • thrombolytics(fibrinolytics) = DISSOLUTIONofalreadyformedthrombus
Anticoagulants • DRUGS ARTIFICIALLY INDUCING “DISTURBANCES“ OF BLOOD COAGULATION • GOAL: TO PREVENT THROMBOSIS OR TO STOP PROGRESSION OF ALREADY FORMED THROMBUS
HEPARIN • UNDIRECT INHIBITOR OF THROMBIN • SUBSTANCE OWN TO BODY (MAST CELLS), USED FROM 1916 • MW = 3 - 30 000 D (15 000 D) • produced from intestinal mucosa of porcine or cattle lungs => qualified in IU • heterogenous anion mucopolysacharid – the strongest organic acid in organism • ACTIVITY IS DEPENDENT FROM THE PRESENCE OF A N T I T H R O M B I N III.
Mechanismofactionofheparin - + 1000x H inactivates already activovated coagulation factors IIA, IXA, XA, XIA
Effectsofheparin • anticoagulant – IIA = inactivation of thrombin (bleeding manifestation) • antithrombotic – XA = inhibition of thrombin formation • inhibition of platelet function - adhesivity and aggregation • stimulation of fibrinolysis • releasing of lipoproteinic lipase clearing of lipemic plasma anticoagulatef. anti - IIa : anti -Xaantithromboticef. 1 : 1
Advantagesofheparin • acts very fast or immediately, but shortly • has massive effect • it has effective antidote, 1 ml protamine binds 100 IU H
Disadvantagesofheparin • only injection (i.v., s.c.), • i.m. – no, irregular absorption and haematoma • T1/2 is variable, prolonged with dose, 3 times per day s.c. • unpredictable anticoagulant effect – wide variability (for different binding to proteins and unpredictable BD at s.c.) • possibility of disease reactivation after stopping administration (rebound efect) • control:APTT (reflexts effect to thrombin) – extension to 1,5-2,5 x of norm
Indicationsofheparin • Th. of deep vein thrombosis and pulmonary embolia • Prophylaxis of vein thrombosis • Prevention of coronary thrombosis (AP, IM) • AIM without TL • Atrium fibrillation • Obturation of peripheral arteries • Hemodialysis, DIC
ADR ofheparin • Bleeding • H. inducedthrombocythopenia(HIT) – lessserious, earlyf.; more seriousf. after5 and days occurenceofthrombosis • Allergy • Reversiblealopecia • Osteoporosisatlong-termuse
LOW-MOLECULAR-WEIGHT HEPARINS (LMWH) • INDIRECT INHIBITORS OF THROMBIN • small molecules, MR 5 000 D • INHIBIT MORE ANTI-XA • PRODUCED BY CHEMIC OR ENZYMATIC DEPOLARISATION OF H • ACTIVITA DEPENDS ON THE PRESENCE OF A N T I T H R O M B I N III
Methodsof LMWH production • depolymerisation • kyselinou dusitou • hydrolysis • heparinisation • irradiation • isolationoflow-molecularfraction • jellyfiltration • ultrafiltration • alcoholextraction
Mechanismof LMWH action anticoagulat. ef.anti - IIa : anti -Xaantithromboticef. 1 : 2 - 4
FONDAPARINUX • INDIRECT INHIBITOR OF THROMBIN • SYNTHETIC PENTASACHARID SPECIFICALLY INHIBITING FACTOR XA • MR = 1 700 D • activity depends on the presence of A N T I T H R O M B I N III • 300X ability to inactivate f. XA
Advantagesoffondaparinux • doesn´t have long chain needed to binding to f. IIA doesn´t inhibit thrombin of bleeding complications also than LMWH • administered s.c. • long duration of action • highly predictable effect • doesn´t influence aggregation of platelets doesn´t induce thrombocythopenia • disadvantage = price
HIRUDIN, BIVALIRUDIN • DIRECT INHIBITOR OF THROMBIN • SPECIFICALLY IRREVERSIBLYINACTIVATES THROMBINWITHOUT NEED OF AT III PRESENCE • IS NATURAL INHIBITOR OF BLOOD COAGULATION GAINED FROM LEECH (HIRUDO MEDICINALIS) • PRODUCED BY DNA RECOMBINANT TECHNOLOGY
MA HIRUDINIS BIND TO THROMBIN AND irreversibly FORMS INACTIVE COMPLEX BIVALIRUDIN-synthetic fragment of thrombin - reversible inhibition of thrombin - duration of action cca 25 min.
Advantagesofhirudin • doesn´t bind to plasma proteins predictable anticoagulant effect • indicated for patients with thrombocythopenia after heparin with need to th. • inactivates not binded, but also thrombin binded to fibrin in thrombus anticoagulant effectivity • inhibits formation of fibrin • inhibits activation of thrombocyts = antiaggregatory effect • prevents activation of f. V, VIII, XI and XIII • peg-hirudin – 1 times per day, s.c.
COUMARINS • I N D I R E C T p.o.ANTICOAGULANTS = ANTAGONISTS OF VITAMIN K factors II., VII., IX., X. DOESN´T ACT ANTICOAGULATORY IN VITRO • DISCOVERED ACCIDENTALLY – LIVESTOCK ATE FERMENTED SHAMROCK– SUBSTANCES IN IT CAUSED DEFICIENCY OF PROTHROMBIN– ANIMALS WERE BLEEDING • Otheruse– poisonforgnawer
MA warfarin • inhibition of epoxidreductase, no formation of vitamin K active form no activation of -carboxylase and no carboxylation of -glutamin residuums of factors II., VII., IX., X. + inhibition of protein C and S carboxylation • coumarins antagonise liver synthesis of f. II, VII, IX and X => • formed are incomplete, unfunctional molecules, which don´t cause coagulation
Pharmacokineticofwarfarin • 100% BA, 99% binding to plasma proteins small distribution volume + long plasma half-life=>many interactions • EFFECT STARTS WITH LATENCY 12-24 HOURS, MAXIMAL EFFECT AFTER 2-3 days • AFTER SECESSION effect REMAINS 4-5 days
DISADVANTAGES ofwarfarin • starting and remaining of effect after secession withlatency (2-3days) • no therapy of a c u t e conditions => prophylaxis • Control of therapy and dosage according to INR (2,0-4,5– according to indication) • Controls of INR v stabilized condition each 3-4 weeks
INR • International normalised ratio patient´s Quick time • INR = Quick time of standard • Prophylaxis of thrombosis INR = 2,0 – 2,5 • Therapy of thrombosis INR = 2,0 – 3,0 • At pat. with antiphospholipid sy. • INR = 3,0 – 4,5
Interactions of Warfarin • pharmacokinetic • high binding to plasma proteins • metabolised with CYP 450 • pharmacodynamic - groceries with high amount of vitamin K, can reduce effect - antibiotics that suppress bacterias in GIT that produce vitamin K (3rd generation of cephalosporins), can increase effect