Hyponatremia
Hyponatremia. Why hyponatremia important ?. Common electrolyte abnormality- inpatient and outpatient Up to 15 % of inpatients 1 Acute- 8.4% in childen 55% in adults Chronic 14-27% 1. Baylis PH. Int J Biochem Cell Biol . 2003;35:1495-1499. Important cause of mortality

Hyponatremia
E N D
Presentation Transcript
Why hyponatremia important ? • Common electrolyte abnormality- inpatient and outpatient • Up to 15 % of inpatients 1 • Acute- • 8.4% in childen • 55% in adults • Chronic • 14-27% 1. Baylis PH. Int J Biochem Cell Biol. 2003;35:1495-1499.
Important cause of mortality • Mortality more if hyponatremia develops after hospitalisation • Increased duration of hospital stay • Increased mortality continues even after discharge • Even mild hyponatremia though till now considered benign is associated with osteoporosis and fractures Adrogué HJ. Am J Nephrol. 2005;25:240-249 Gill ,clin endocrino 2006 Clayton ,QJM 2006 European Jr of Endocrinology,2010 Manisha
Definition of Hyponatremia • Normal serum sodium level : 135 – 145mEq/L • Hyponatremia is defined as a serum sodium level less than 135mEq/L • Severe - serum Na < 120mEq/L
Clinical Manifestations • Hyponatremia not a disease but a manifestation of a variety of disorders. • Clinical symptoms • hyponatremia itself • Disease causing hyponatremia recognition of hyponatremia incidental.
Pathogenesis Acute Low serum Na More Na in brain Water enters brain cells Cerebral oedema Chronic Adaptation
Symptoms depend on • magnitude of the hyponatremia • rapidity of its development. Asymptomatic GI sym Headache Lethargy Confusion Obtundation S [Na] > 125 mmol/L or Gradual onset Stupor Seizures Coma Rhabdomyolysis Brain stem compressiom Pulm oedema Na+ level <120mEq/L or Rapid decrease(<48hr)
Symptoms & signs • Gait disturbances • Fractures • reduction in total hip bone mineral density of 0.037 g/cm2 for every 1 mmol/l drop in plasma sodium concentration. European Jr Endocrinology 2010 Manisha Sahay
Etiology -Hyponatremia ? Hyperlipidemia Hyperproteinemia ? ? ? ? Hyperglycemia Mannitol CHF NS Cirrhosis CRF Salt wasting dz RTA Diuretics Cerebral salt wasting GI loss 3rd space loss SIADH GC def Hypothyroid Exercise ind Psychogenic
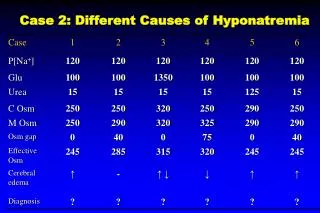
Determine if true Hyponatremia? IA Pseudohyponatremia/Normal plasma osmolality (275-295) • Hyperlipidemia - ion-specific electrodes avoid this • Hyperproteinemia-Multiple myeloma IB Increased plasma osmolality /Translocational/redistributive (osmo > 295) • Hyperglycemia1.6 mEq/L for every 100 mg/dL [glucose) • Mannitol II. Hypoosmolalhyponatremia (serum osmolality<275mOsm/kg)
2 stepcheck volume status Euvolemic Hypervolemic Hypovolemic
Hypovolemic- Low CVPResponds to NS Low urine Na(<20 mmol/l) High urine Na >20 mmol/l Renal Salt wasting nephropathy Mineralocorticoid deficiency-high K Osmotic diuresis-KB Cerebral salt wasting • Non renal • Volume Depletion • GI, lung or skin losses -burns • Third space sequestration • CSW • Excess water intake Step 3 Check renal or non renal Urine Na Manisha Sahay
Diuretics Thiazides • Urine excreted- NS • Lose more salt than loop • Reason for hypoNa • Interfere with urine dilution • Common in elderly females • Occurs within 2-4 weeks • Discontinue diuretics Loop Diuretics • Urine excreted 1/2 NS • Lose > water than thiazides • Reason for hypoNa: • Impair generation of medullary hypertonicity
Cerebral Salt Wasting • Causes: Head injury, surgery, tumors, Infections • Signs/symptoms: • Polyuria, Dehydration/hypovolemia/Hypotension • High urine Na > 20 mmol/L • Pathogenesis: • renal Na loss d/tplasma ANP, BNP • Volume depletion could be protective for ICP • Treatment: • Volume replacement - large volumes of NS • Oral Na supplementation for a period of time Berendes Lancet 1997, Isotani Stroke 1994, Wijdicks Stroke 1991 Mather J Neuro Nsurg Psych 1981; Wijdicks Ann Neuro 1985
TreatmentHypovolemichyponatremia • Isotonic saline Restoration of euvolemia removes the hemodynamic stimulus for AVP release Excretion of the excess free water
Hypervolemic Euvolemic Hypovolemic
Hypervolemic -High CVPIncreased total body water that exceeds the increase in total body Na+ Low urine Na <20 mmol/l High urine Na >20 mmol/l Advanced renal failure • CHF • Cirrhosis with ascites • Nephrotic syndrome Step 3 Check urine Na Manisha Sahayin
TreatmentHypervolemic hyponatremia Restriction of Na+ and water intake • Promotion of water loss in excess of Na+ • Vasopressin antagonists approved for use • Correction of underlying disorder
Hypervolemic Euvolemic Hypovolemic
Euvolemic – Normal CVP Normal sodium stores (N ECF) & total body excess of free water. • SIADH/Reset osmostat • Primary polydipsia • Hypothyroidism • Glucocorticoid deficiency • Exercise induced • Beer potomania • Post op Step 3 All have high urine Na U osm <100 in PP, BP
SIADH (Bartter’s Criteria)60% of all euvolemic hyponatremia Step 4 Check urine osmolality K/Cr/ Cr/Urea/uric acid T3/T4/TSH Cortisol CT as needed • F Essential criteria • Hyponatremia • pl osm<275 • Euvolemia clinical • u osmolality > 200 mOsm/kg • N renal, cardiac, hepatic, adrenal, pituitary, thyroid • No H/o antidiuretic drugs • No emotional or physical stress • Urinary sodium > 20 mEq/l • Cr N, N ABG, K+ handling Supplemental features • uric acid<4 • BUN<10 • failure to correct hypoNa after NS infusion • correction of hypoNa after fluid restriction • S ADH U SP gravity can be used if u osm not possible, U osm 100= u sp gr 1.005 a
Disorders associated with SIADH CNS-ADH secr Encephalitis /Meningitis , trauma Brain abscess/Brain tumors GBS/Acute intermittent porphyria Subarachnoid/subdural hematoma Cerebellar and cerebral atrophy Cavernous sinus thrombosis Neonatal hypoxia Hydrocephalus Delirium tremens CVA, Acute psychosis Peripheral neuropathy Multiple sclerosis Pulmonary Pulmonary abscess Tuberculosis Aspergillosis Positive-pressure breathing Asthma Pneumothorax Cystic fibrosis Lung cancers Cancers Small cell carcinoma of the lung Carcinoma of the duodenum Carcinoma of the pancreas Thymoma Lymphoma Ewing’s sarcoma Mesothelioma Carcinoma of the bladder Prostatic carcinoma Olfactory neuroblastoma PULMONARY CANCERS CNS
DRUGS Antidiuretic hormones: Vasopressin,oxytocin Diuretics: Thiazides,furosemide, CNS-active drugs: Vincristine,carbamazepine, Psychotropic drugs Inhibitors of prostaglandin Chlorpropamide, Salicylates, Acetaminophen, NSAIDS,COX 2 I Others: Clofibrate,Cyclophosphamide, Somatostatin Manisha Sahay
Primary Polydipsia • Psychiatric disorder, thirst with antipsychotics • ±Hypothalamic lesions • No hyponatremia unless intake >10-15 L/d, or acute 3-4 L water load • Urine osm below 100 • Rx: Restrict free water ;classically rapid correction
Reset osmostat • Can excrete water load (10 to 15 mL/kg given orally or intravenously). -excrete more than 80 percent within 4 hours • Mild hyponatremia • No treatment needed Manisha Sahay
Beer protomaniaLow Dietary Solute Intake • Elderly, malnourished (“tea and toast” diets) -poor in solutes (Na/K) • Beer drinkers (high water intake, low protein) • Pathogenesis • Minimum urine osmolarity- 60 mosm/l • At least 600-900 msom/kg/d solute load needed to excrete water >4 l • Beer protomania- daily solute excretion < 250 mosmol /kg, hence maximum urine output can be <4 L day ,if more water ingested -hyponatremia • Urine appears dilute (osm of< 100) • Rx: NS, increased dietary solute
Exercise associated hyponatremia (EAH) Clinical features • May be severe: cerebral edema, non cardiac PE Pathogenesis • H2O excess; impaired renal H2O excretion • Nonosmolar AVP release esp if water in >out Treatment • Limit water to 400-800 ml/h; drink only when thirsty • No role of NS, 3% Nacl if severe JCEM 2008;93:2072-78
Investigations History & volume status Serum Osmolality Urine Osmolality/sp gr Urine Na S Cr/urea/K T3/T4/TSH CXR CT Scan Manisha Sahay
Hyponatremia Step1 S osmolality N 275-295 Hyperlipidemia Hyperproteinemia Low<275 True High>295 Hyperglycemia Mannitol Step 2 Volume High Hypovolemic Euvolemia Step3 Urine Na Step 3 Urine Na Step 4 U Osm/TSH/GC < 20 mmol/l CHF NS Cirrhosis >20 mmol/l CRF Renal Salt wasting dz RTA Diuretics Cerebral salt wasting Extra renal GI loss 3rd space loss SIADH GC def Hypothyroid Exercise ind Psychogenic
Treatment –Euvolemic Hyponatremia Manisha Sahay
Hyponatremia Asymptomatic Symptomatic Chronic Acute <48 hrs Chronic>48 hrs Some immediate correction Hypertonic saline + Furosemide Change to water restriction Frequent serum & urine electrolytes Do not exceed 12 meq/l/d No immediate Correction needed Emergency Hypertonic saline+ furosemide Long term management Treat etiology Water restriction Demeclocycline Urea V2 receptor antagonist Thurman et al,Therapy in nephrology and Hypertension,Saunders 2003
Therapeutic Strategy Euvolemic hyponatremia • Treatment varies with • Presence or Absence of Symptoms • Duration • Magnitude of Hyponatremia • Risk for neurological dz- young, females, elderly,menstruation
Acute/Severe/symptomatic hyponatremia Manisha Sahay
Rate of correction of hyponatremia • Acute • severe (S Na+ <115mmol/L) • symptomatic • Hypertonic (3% NaCl) • 0.5 mmol/l/hr or 12 mmol/l/day • Stop • if convulsions subside • if S Na 120 mEq/L Kumar S, Berl T. The Lancet 1998; 352: 220-8 Adrogue HJ, Madias NE. NEJM 2000; 342: 1581-9
Fluids for correction Ringer’s = 130 mEq/L 0.45%NS = 77 mEq/L • 3% NaCl- 513 meq/L 0.9% NaCl- 154 meq/L
Total correction in 12 hrs = 6 mmol • Volume of infusate needed = B Wt X 0.6 X Desired increment in Na (120-114) Infusate Na X 1.5 • 50 kg • 50X 0.6x6 = 0.23 litre or 230 ml 513X1.5 230 ml in 12 hours 19 ml/hr
Symptomatic/chronichyponatremiaGradual correction Manisha Sahay
Chronic symptomatic>48 hrs • 3% NaCL • < 0.5 to 1.0mmol/L per h • (<10 to 12mmol/L over first 24h) • Water restriction Chronic asymptomatic > 48 hours • No immediate correction • Water restriction Manisha Sahay
Long term management Euvolemic hyponatremia • Water restriction • Free water restriction ,¾ maintenance (1 L/d) • Clozapine -schizophrenic patients with compulsive water drinking • Pharmacological agents (Long-term) • Demeclocycline 300 - 600 mgbd • Urea 15-60 gm/d • Lithium • V2 receptor antagonist- Aquaretics
AVP Receptor antagonists – • Mechanism of action Bind to the V2 receptors in renal collecting tubules/ducts Vasopressin antagonist Uses • Euvolemic/ hypervolemic hypo Na+; Contraindicated in hypovolemia • Chronic hyponatremia not in acute hyponatremia or in patients with sNa < 115 mmol/L as slow aquaresis Adverse effects: Thirst ; dry mouth SALT NEJM 2006
Vasopressin Receptor Antagonists *SALT I and SALT II Trials.
CI • Concomitant use of vaptan and potent CYP3A4 inhibitors such as ketoconazole, itraconazole, clarithromycin, ritonavir, or indinavir is contraindicated Manisha Sahay
Central Pontine MyelinolysisOsmotic demyelination • Pathogenesis • rapid correction / overcorrection of ch hyponatremia. • hypoxic encephalopathy / complication of therapy • Prevention • Adequate oxygenation • Gradual increase in serum sodium level to 120-125 mEq/L. • Symptoms • Dysarthria, dysphagia, seizures, altered mental status, quadriparesis, hypotension ,locked in syndrome, extrapontine • Begin 1-3 days after correction of S Na • Irreversible , devastating • MRI diagnostic < 24 h • Risk factors- Hypokalemia, females,alcoholism, liver transplant • Treatment- Relowering S Na - hypotonic fluids, Desmopressin dsMsh S
Summarising…… Manisha Sahay
Hyponatremia S osmolality N 275-295 Hyperlipidemia Hyperproteinemia Low<275 True High>295 Hyperglycemia Mannitol Volume High Hypovolemic Euvolemia Urine Na Urine Na Urine Osm, S Cr,Ur,TSH < 20 mmol/l Extrarenal CHF NS Cirrhosis >20 mmol/l Renal CRF Renal Salt wasting dz Diuretics Cerebral salt wasting Extra renal GI loss 3rd space loss SIADH GC def Hypothyroid Exercise ind Psychogenic
Hyponatremia Asymptomatic Symptomatic Acute <48 hrs Emergency No immediate Correction needed Long term management Hypertonic saline Go slow
Take home message • Hyponatremia –a common, life theatening problem • Step wise evaluation important • Inappropriate treatment – Worse than disease Practising is the best way of learning!!! Manisha Sahay