Positive Youth Development
By John Fishburn, adapted from Robert Smedley and Jeff Styer. Positive Youth Development. Quiz: Who said “No Man is an Island?”. ANSWER. John Donne Meditation XVII from Devotions Upon Emergent Occasions 1624 Picture From http://www.luminarium.org/sevenlit/donne/. ECO-MAP.

Positive Youth Development
E N D
Presentation Transcript
By John Fishburn, adapted from Robert Smedley and Jeff Styer Positive Youth Development John Fishburn and Jeff Styer
ANSWER • John Donne • Meditation XVII from Devotions Upon Emergent Occasions 1624 • Picture From http://www.luminarium.org/sevenlit/donne/
Objectives of Module # 1To Understand: • The Positive Approach to Youth Education • The idea of Resiliency • Positive Approach to Preventing Development Problems • Resiliency • Assets • Protective Factors • Risk Factors Robert Smedley Wayne/Homes MHRB
Resiliency Resiliency is the key social/emotional element in the positive approach to education and problem behavior prevention. • Resiliency is a strengths based solution. • Resiliency is the opposite of a problems based solution. Robert Smedley Wayne/Homes MHRB
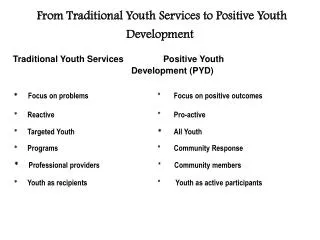
Resiliency is the Positive Alternative Traditional Prevention and Treatment Approaches have focused on the negative. They have been designed to identify and stop problems. These approaches: • Tend to suggest that the negative value is greater than the positive. • Tend to promote view that world/community events are not good. • Tend to label groups as negative – the troubled kids • Tend to label individual youth as “bad”. • Tend to focus people on problems rather than building positives in their lives. • Time spent focusing on problems limits the amount of time spent on building for the future. This approach does not lead to change. Robert Smedley Wayne/Homes MHRB
Resiliency The basic idea behind the positive approach to youth education and development is the finding that human beings often prosper and thrive in difficult and dangerous situations. Youth/Humans who are able to thrive is these situations have been discovered to have: • Social/emotional assets • Protective factors which foster this abilityto succeed Despite all odds that they should not do so. Robert Smedley Wayne/Homes MHRB
Resiliency is focusing on the positive The idea that youth who are resilient, can thrive in difficult situations has lead to the approach of designing programs to reinforce the development of: • Assets (developmental) • Protective Factors • Risk Factor Reduction Strategies Robert Smedley Wayne/Homes MHRB
Social/Emotional Assets, also called Developmental Assets Asset Development Theory was founded by the Search Institute of Minneapolis, Minnesota – Lutheran Brotherhood Foundation. • Asset Development Theory holds that there are an array of internal and external assets common to all “thriving” human beings in our western culture. • Assets are seen social/emotional building blocks available to all youth regardless of social class. • The Search Institute has identified 20 of the internal and externals for their work. Robert Smedley Wayne/Homes MHRB
Asset Development Theory • Holds that the more assets that a youth has, the less likely they will become involved in any one or more of the common litany of self destructive behaviors of our day, i.e. drugs, promiscuity, anti-social activity, school failure. • Is cumulative, not linear. This means that success related to being asseted is related to the amount of assets you have, not a linear correlation between one asset and one prevented behavior. • Is a programmatic strategy, in which the specific design of programs is to increase the assets of the young persons in an age appropriate fashion. • Youth lose assets as the mature, thus strategies are ongoing in order to match their maturation with new strategies. Robert Smedley Wayne/Homes MHRB
40 Developmental Assets • Developmental Assets are External and Internal • Grouped into 8 categories • External include: Support, Empowerment, Boundaries and Expectations, and Constructive Use of Time. • Internal Include: Commitment to Learning, Positive Values, Social Competencies, and Positive Identity.
Age Specific • The Developmental Assets are a little different for different Age groupings • Early Childhood – Ages 3 – 5 • Middle Childhood – Ages 8 – 12 • Adolescence – Ages 12 – 18
Asset Examples Asseted: A youth involved with their family. The family regularly takes dinner together . The whole family participates in extracurricular school activities, family projects in the community. The youth is involved with adults other than their parents; and participates in the planning and development of activities in the community and church. Home life is safe (outsiders, computer predators) and well regulated allowing for quiet study and creative time Under Asseted A youth, junior high aged or older has not set goals. He/she spend most of their time alone at home in their home or out with friends. The youth is not currently involved with any clubs or social activities at school The youth has no hobbies or interest in community activity. The youth is highly externalized (focused on events outsides of self and family) spends most of their time reflexively, responding other controls. Tends to be vulnerable to “drug” or risk stimulus Robert Smedley Wayne/Homes MHRB
SO WHAT? As assets increase profound reductions occur in the health compromising behaviors and increase the thriving outcomes. Developmental assets are strongly linked to GPA and to actual grades in English, science and mathematics (Benson, p 32). Students who report a high number of assets (31-40) are two times more likely to report getting mostly A’s in school compared to students with 11-20 assets and about 8 times more likely than those reporting 10 or fewer assets (p 32).
Which Assets can YOU impact? • You are a Teacher • You are a Community Member • You are a Neighbor • You are an Adult Role Model
PROTECTIVE FACTORS The Protective Factor approach to resiliency is an environmental approach similar to asset development and is built on the ideas that: • Youth with a positive protective factor balance are more likely to thrive than those who do not. • Protective factors are available to all youth. • Protective Factors can be built into an environment programmatically. Robert Smedley Wayne/Homes MHRB
Protective Factors • Sense of Humor. • Sense of Well Being. • Access to quality pediatric/adolescent health care • Access to quality mental health care • Community norms against violence. • Community norms against crime • Residential stability • Constant age appropriate discipline • Adult monitoring and supervision • Family problem solving ability. • Parent-teacher cooperation • School to work transitions programs • Friends, peers wo do not engage in problem behavior A complete list of Protective factors can be found in the appendix to this power point Robert Smedley Wayne/Homes MHRB
Protective Factor Example The Protective Factor approach is built on a fundamental belief in the human ability to be resilient. An example of a protective factor taking effect is: • A child/family is able to access to quality pediatric/adolescent health care. As a result the child receives all the important immunizations, and the parents learn good nutrition, exercise and rest practices for their child. • The child experiences normal brain and body development and enters school with a general sense of well being that is reinforced by their ability to learn quickly and complete in school activities. • The child educational baseline (memory) of school is positive and is naturally reinforced by continuing to eat, sleep and interact well with peers. • This protective factor is linked with the child’s immediate and long term success at school. Robert Smedley Wayne/Homes MHRB
Risk Factors Risk Factors: These are the environmental conditions which the “Protection”. The fundamental belief with risk factors holds that: • Risks can be identified • Risks can be reduced and controlled. • Protective factors provide immunity, or inoculation to risk “infection”, but they do not necessarily prevent exposure. Robert Smedley Wayne/Homes MHRB
Risk Factors • Availability of drugs • Availability of firearms • Community norms that tolerate crime • Low neighborhood attachment • Transitions and mobility • Lack of relationship skills • Parenting: lack of appropriate discipline • Family violence • Anti-social behavior • Lack of commitment to work • Alienation A complete list of Protective factors can be found in the appendix to this power point Robert Smedley Wayne/Homes MHRB
Risk Factor Example The idea of Risk Factors is built on a fundamental belief that the environment can shape human behavior. An example of reducing risk factors for a positive effect is: • A family with a young child has a family economy that requires the family to move frequently, thus causing their child to switch from school district to school district. • The parents learn that children often fail at school due to the difficulty involved switching classes, in making new acquaintances and getting involved in healthy activities in different schools and communities. These are risk factors. • The parents develop a routine of enrolling their child in school, meeting the teachers to develop a classroom transition plan and getting their child involved school/community social interactive programs when they move to new districts. These are Protective Factors. • Their child learns a process of adapting to new situations even though the risk of falling out of the system is great. Robert Smedley Wayne/Homes MHRB
Positive Action • Evidence-Based Program designed to teach youth about character, values, and decision-making. • Age specific using a variety of teaching methods • Highly interactive and easy to use • Offered by Tri-County ESC and Transitions PLUS program Robert Smedley Wayne/Homes MHRB
Alcohol and Drug Use, Abuse and Addiction A Safety and Violence Prevention Curriculum Module Three Robert Smedley Wayne/Homes MHRB
Fact: Alcohol (Ethanol) is flammable, and toxic; it is used as fuel and sanitizer and affects every organ in the body. Alcohol is a depressant and illegal if under 21! Fact: Marijuana: (Cannabis) is a hallucinogen and causes hallucinations and memory problems; it is illegal! By John Fishburn, Transitions Coordinator Teenage Alcohol and Marijuana Use
Teenage Alcohol Problems • Teens tend to “binge” drink (drink a lot all at one time). • This is a leading cause for teenage alcohol death; “accidents” are the #1. • Teens often drink with friends at big parties where other drugs are involved • Mixing alcohol with other drugs can drastically increases chance of death!
Wine coolers are just as dangerous as any other form of alcohol. Alcohol companies target youth with these products. They are sweetened, flavored, and marketed to hide the poisonous taste of alcohol!
Heavy marijuana use is associated with lingering brain effects even a day after quitting. Marijuana sticks in your body and is hard to get rid of! Marijuana: weed, pot, ganja, hash, bud, 420, wacky tobaccy
Myth: You can’t get addicted to marijuana. Fact: Regular marijuana use does lead to chemical addiction! Myth: Marijuana can’t kill you. Fact: Marijuana is more cancerous than tobacco! If marijuana is mixed with alcohol, it is more likely to cause alcohol poisoning! Myth: Marijuana is a natural herb. Fact: There are many poisonous ‘natural’ herbs, plus, you NEVER KNOW what else is mixed in with it! A lot of street-bought marijuana is mixed with speed, meth, or other dangerous drugs!
90.1% of 8th graders DID NOT use marijuana at all during the past year! 78% of 8th graders DID NOT drink any beer, wine coolers or liquor during the past year! 81.4% of 8th graders DID NOT smoke cigarettes at all during the past year! Most drug use occurs on the weekends with friends. 2007 Wooster PRIDE Survey:
Here’s What We Know…2007 PRIDE Survey Data: • In the past year, what percentage of Wooster 12th graders report using … • Marijuana? 23% • Beer? 48% • Wine Coolers? 43% • Liquor? 45% • Cigarettes? 20%
What percent of WHS students did NOT drink alcohol in the past 30 days? (67%)What percent of WHS students did NOT use marijuana in the past 30 days? (85%)What percent of WHS students drink beer if their friends think it is wrong? (2.9%)WHS drink beer more or less than the high school students nationally? (less, by 6%)
All Non Medical Chemical (substance) Use by Children is Drug Abuse. Illegal Chemicals which alter moods and cognitions are commonly referred to as drugs.Many of these substances are used obsessively. These include: • Alcohol • Tobacco • Caffeine • Medications taken from family or friends medicine cabinets. These can include mood depressors or elevators. • Marijuana • Cleaning chemicals such as oven cleaners, gasoline or other solvents • Cocaine • Hallucinogenic • Stimulants (methamphetamine) • Opioid (Pain Relievers) Robert Smedley Wayne/Homes MHRB
To say that a chemical alters Moods or Thoughts means that the chemical alters the neuro chemical activity of the brain.Brain Neuro Chemicals are all involved with Learning. Non Medically Monitored Drug use can impair learning on both the Social/Emotional and Cognitive levels. This makes substance use an educational issue. Robert Smedley Wayne/Homes MHRB
Behavior Change in Jr. High or Middle School Students is Rapid. This is because of: • The Onset of Sexual Development –Puberty. • The increased need to compete and succeed with peers for status (peer pressure). • The decreasing influence of the family on youth behavior decisions Robert Smedley Wayne/Homes MHRB
“Some” Changes is Student Behavior Signals Distress. • Maturation and the emotional chemical changes in the Brain may cause depression or anxiety disorders. • Students without adequate family or social supports are vulnerable to this distress • Youth who experience social/emotional failure during this period may turn to peer groups who are experimenting with high risk relief and escape behaviors Robert Smedley Wayne/Homes MHRB
CORRESPONDINGLY • Substance abuse, that is alcohol, tobacco, Caffeine, Marijuana, Stimulants, increases by as much as 1200% during the middle school years. • This parallels and complements the sexual and peer related behavior changes. Robert Smedley Wayne/Homes MHRB
General Indicators of Distress • School work has declined; grades slip and drop suddenly • Missing school (skipping secretly or being too “tired” or “sick” to attend). • Unexplainable, dramatic mood changes (irritable, moody) • Dropping out of usual activities (music, sports, hobbies). • Seems to have lost motivation. • Changes in general, significant interests. Robert Smedley Wayne/Homes MHRB
General Indicators of Distress • Depressed or anxious “affect”. • Decrease in “happiness and well being”. • Forgetful. • Unusual sleeping habits (changing over time or dramatically). • Increased risk taking (involvement with risk factors. Robert Smedley Wayne/Homes MHRB
Warning Signs of Alcohol and Drug Use (Continued) • Fascination with drugs displayed in sub cultural language, symbology on tee shirts, clothing • Paraphernalia in room (posters, pipes, clips) • Show negative, argumentative, paranoid, confused, destructive, or anxious behavior. • Act rebelliously • Show drastic weight loss or gain. • Always needs money, or has more money that they should • Smoking tobacco. Robert Smedley Wayne/Homes MHRB
Preventing and Treating Substance Abuse • The importance of preventing substance abuse during the teen years is in the relationship between Teen use/abuse and the development of substance dependency later in life. • Delaying the Onset of use or abuse until the third decade of life reduces the probability of addiction by significantly. • This is related to the physical development of the brain. Robert Smedley Wayne/Homes MHRB
Prevention • Youth Substance Abuse is not inevitable, even in the most high use areas. • Strategies have been developed that demonstrated predictable prevention of abuse and dependency. • These strategies are referred to as Evidence Based Prevention. • Information about them is available for study on the SAMHSA website https://preventionplatform.samhsa.gov/Macro/CSAP/dss_portal/Templates_redesign/start.cfm Robert Smedley Wayne/Homes MHRB
Principles for Preventing Drug Use Among Children and AdolescentsNational Institute of Drug Abuse • Prevention programs should be designed to enhance "protective factors" and to move toward reversing or reducing known "risk factors." • Prevention programs should target all forms of drug use, including the use of tobacco, alcohol, marijuana, and inhalants. • Prevention programs should include skills to resist drugs when offered, strengthen personal commitments against drug use, and increase social competency (e.g., in communications, peer relationships, self-efficacy, and assertiveness) in conjunction with reinforcement of attitudes against drug use. • Prevention programs for adolescents should include interactive methods, such as peer discussion groups, rather than didactic teaching techniques alone. Robert Smedley Wayne/Homes MHRB
Prevention Principles Continued • Prevention programs should include a parents' or caregivers' component that reinforces what the children are learning, such as facts about drugs and their harmful effects. Moreover, the intervention should promote opportunities for family discussions about use of legal and illegal substances and family policies about their use. • Prevention programs should be long term and should continue over the school career, with repeated interventions to reinforce the original prevention goals. For example, school-based efforts directed at elementary school and middle school students should include booster sessions to help with critical transitions from middle school to high school Family-focused prevention efforts have a greater impact than strategies that focus on parents only or children only. • Community programs that include media campaigns and policy changes, such as new regulations that restrict access to alcohol, tobacco, or other drugs, are more effective when they are accompanied by school and family interventions. Robert Smedley Wayne/Homes MHRB
Prevention Principles Continued • Community programs need to strengthen norms against drug use in all drug use prevention settings, including the family, school, and community. • Schools offer opportunities to reach all populations and also serve as important settings for specific subpopulations at risk for drug use, such as children with behavior problems or learning disabilities and those who are potential dropouts. • Prevention programming should be adapted to address the specific nature of the drug use problem in the local community. • The higher the level of risk for the target population, the more intensive the prevention effort must be, and the earlier it must begin. • Prevention programs should be age-specific, developmentally appropriate, and culturally sensitive. • Effective prevention programs are cost-effective Robert Smedley Wayne/Homes MHRB
Treatment Programs Vary for Abuse, Addiction and Physical Dependencies • Treatment Programs are designed around need. • They include assessments, individual and group counseling, urinalysis, intensive counseling and education, long term residential, medical care. • Assessments may or may not include psychological diagnosis. • The duration of treatment programs vary from brief therapy to long term care. • Addiction Treatment often involves medical care in addition to psycho/social interaction. • Treatment works best when the whole family is involved. Robert Smedley Wayne/Homes MHRB