Pay-for-Performance in Nursing Homes: Enhancing Quality of Care
190 likes | 326 Vues
This presentation by Rachel Werner explores the Pay-for-Performance (P4P) model in nursing homes, emphasizing how aligning financial incentives with quality of care can transform healthcare outcomes. Currently, payment systems prioritize quantity over health quality, hindering progress towards improved resident health. P4P programs reward providers for achieving specific performance targets across several metrics, including staffing levels, resident satisfaction, and compliance. The presentation also discusses the effectiveness of P4P in impacting health disparities and outcomes compared to traditional hospital systems.

Pay-for-Performance in Nursing Homes: Enhancing Quality of Care
E N D
Presentation Transcript
Pay-for-Performance in Nursing Homes SUMR Presentation Mentor: Rachel Werner
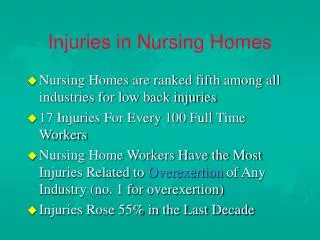
Theory • People respond to incentives. • Current system: payment based on services/quantity, not health/quality • Final goal of health care system: improve health • Under P4P: Providers are rewarded for meeting pre-established targets in quality of care they deliver
Nursing Home Residents 2006: 1,375,661 Nursing Home Residents
States with P4P NH Program Red = Currently running P4P Pink = Planning
Types of Measures • Staffing Levels • Clinical Measures • Resident Satisfaction • Administrative Costs • Medicaid Utilization Ratio • Deficiencies
Models for Financial Incentives • Attainment – establish a target level of performance (Payment > 80% Staff Retention) • Ranking – measures performance against other providers (Payment > top 10%) • Improvement – Payment for achieving improvement over previous period. • Continuous – Payment each time appropriate care is delivered.
Iowa Started: July 2002 • Deficiency-free survey (2 pts) • Regulatory compliance with survey (1 pt) • Nursing hours provided (2 pts max) – 2 pts for >75 percentile • Resident satisfaction (1 pt) - >50th percentile • Resident advocate committee resolution rate (1 pt) - > 60th percentile • High employee retention rate (1 pt) - > 50th percentile • High occupancy rate (1 pt) – at or above 95th • Low administrative costs (1 pt) - >50th percentile • Special licensure classification (1 pt) • High Medicaid utilization (1 pt) - > 50th percentile • 7 pts and higher: 3% increase in daily per diem reimbursement raet. • 5-6 pts: 2% increase • 3-4 pts: 1% increase
Bigger Question • Does P4P affect health outcomes in nursing homes? • Difference between Nursing Home and Hospitals? • Effect on health disparities?
The Road to Universal Health Care:A Look at Singapore Mentor: Arnold Rosoff
Singapore • A rich history of public-funded health • A strong Confucian philosophy • Solidarity
Consumer-Directed Health Care • The Republican “Ace in the Hole” • Focuses on individual responsibility • A free market solution for health care • Competition – drives down prices • Individual Choice – eliminates moral hazard
The Singapore Model • Medisave (Medical Savings Accounts) • 6 – 8 % of income is placed in a personal MSA. • Administered by the Central Provident Fund (CPF) • Rolls over from year to year • Medishield (Catastrophic Medical Insurance) • Vast majority of Singaporeans buy in. • Low premiums, widely transparent benefits • Other ‘safety nets’ • Eldershield • Medifund
The Singapore Model • Lowering Costs: Moral Hazard or Rationing? • Limits on everything: from drugs to MSA withdrawals • Moral Hazard Myth? e.g. Hospital Wards • Responsibility: Individual or Family? • MSA funds – cover immediate family members
Additional Issues • Means Testing • Screening applicants based on income/wealth to determine subsidies • Very unpopular – hot political issue • Health Disparities • Haves vs. Have-nots? • Rise of private insurance • Adverse selection
Singapore: A Model for the US? • Distrust in the government • Focus on individual • Unwillingness to ration
Special thanks to the following people for their generous support: • The University of Pennsylvania Provost’s Diversity Fund • The Center for Health Equity Research and Promotion (CHERP) • Pennsylvania Department of Health Office of Health Equity • Arnold Rosoff and Rachel Werner • SUMR and LDI