Download
1 / 47
580 likes | 1.67k Vues
Adjuvant Systemic Treatment: Personalized Management of Breast Cancer. Dr. Law Siu King Department of Surgery United Christian Hospital. Why do the patients with operable breast cancer receive adjuvant systemic therapy? . Role of adjuvant therapy for operable breast cancer.

E N D
Adjuvant Systemic Treatment: Personalized Management of Breast Cancer Dr. Law Siu King Department of Surgery United Christian Hospital
Why do the patients with operable breast cancer receive adjuvant systemic therapy?
Role of adjuvant therapy for operable breast cancer • Systemic adjuvant treatment is used to tackles the micrometastasis and that accounts for most of the improved survival for operable breast cancer patient seen in the last few decades.
Current evidences of benefits of adjuvant endocrine therapy • Tamoxifen • It has been shown Tamoxifen for about 5 years reduced the risk of recurrence by 11.8% and the absolute risk of death by 9.2%.1 Recurrence↓11.8% Mortality↓9.2% 1. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG)*Lancet 2005;365:1687-1717
Current evidences of benefits of adjuvant endocrine therapy • Aromatase inhibitors • AIs (letrozole and anastrozole) have each been shown to improve DFS compared with tamoxifen when given as first line adjuvant therapy for a planned 5 years in postmenopausal women with hormonal receptor-positive early breast cancer 1,2. 1.BIG 1-98 Coatest et al J CLin Onco 2007 2. ATAC trial Forbes JF et al Lancet Onco2008
Current evidences of benefits of adjuvant chemotherapy • NSABP B20 study2, for early breast cancer patient with pathology result of ER +ve & Node –ve who were treated with chemotherapy and hormonal treatment, 4% of patients benefited from the additional of chemotherapy. 11% has recurrencedespite having chemotherapy and 85% were disease free regardless of chemotherapy. Fisher et al. J Natl Cancer Inst 1997;89:1673-82
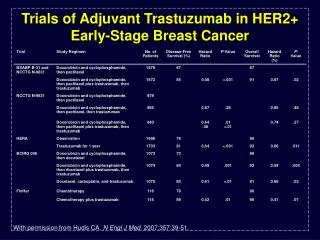
Current evidences of benefits of adjuvant targeted therapy • Adjuvant Transtuzumab ( Herceptin) has been shown to be a major factor in improving survival from HER2-Positive Breast Cancer1,2,3 ↑ HERA trial, absolute benefit for DFS 8.4 % ↑ at 2 yr 1.HERA Piccart-Gebhart, NEJM 2005 2.Romond EH et al. NEJM 2005 3.Smith Et al Lancet 2007
Adjuvant Systemic Treatment for Breast cancer • General principle adjuvant treatment decisions are based on the balance among • risk of relapse, • proven survival benefits of treatment, and • the costs and toxicities of treatment, as well as • on patient preference and co-morbidities.
Determinants of prognosis • For many years , the primary determinants of prognosis included ER, PR and HER2 status, histology, grade, tumor size and axillary LN status.
Prognostic tools • Nottingham prognostic Index( NPI) has been used for many years. Itis based 3 factors using the following formula: • NPI=p tumor size (cm)x0.2+LN stage +histological grade • LN stage( score 1,2 or 3 with 1 =node negative , 2= 1-3 involved nodes and 3 =more then 3 nodes), histological grade ( score 1,2, or 3) + histological grade • Arbitrary cut-off points of 3.4 and 5.4 are used to divide patients into 6 prognostic groups: excellent, good, moderate I and II, Poor and very Poor
Prognostic tools • Other pathology based prognostic tool used in breast cancer included • Adjuvant!Online • Adjuvant! Online can be accessed at www.adjuvantonline.com. • It is a decision tool for assessing the risks of an individual patient developing recurrent disease and/or dying within 10 years, when receiving specific treatment on the basis of well validated factors • Age, comorbidities, LN status, Tumor size, tumor grade and hormonal receptor status • St Gallen Criteria
St. Gallen Consenus • St. Gallen derived algorithm for selection of adjuvant systemic therapy for early breast cancer patients includes • Tumor size and grade • Nodal status, • Menopausal status, • Peri-tumoral vessels invasion • Endocrine status and • HER 2 status. St. Gallen Expert Consensus Meeting 2007
Case Study Madam Choi, 59/F, Excellent Good Past Health Has newly Dx CA Left breast ,presented with left breast mass , Confirmed by imaging (MMG/ USG) and histology (Core Biopsy) WLE + Sentinel lymph node biopsy Pathology: Primary tumor - 2.2cm ,Grade 2, invasive ductal carcinoma, clear resection margins ER 300(+++), PR 300(+++), cerb2 –ve. No lymphovascular invasion Sentinel lymph nodes – 0/2 Stage IIA (pT2 N0M0) What adjuvant systemic therapy should the patient receive? Should the patient receive chemotherapy?
Case Study Madam Choi, 59/F, Excellent Good Past Health Has newly Dx CA Left breast ,presented with left breast mass , Confirmed by imaging (MMG/ USG) and histology (Core Biopsy) WLE + Sentinel lymph node biopsy Pathology: Primary tumor - 2.2cm ,Grade 2, invasive ductal carcinoma, clear resection margins ER 300(+++), PR 300(+++), cerb2 –ve. No lymphovascular invasion Sentinel lymph nodes – 0/2 Stage IIA (pT2 N0M0) Base on the St. Gallen Criteria , She has intermediate risk (T2 and Grade 2 tumor)
Is hormonal therapy alone for her enough ? • Base on NSABP B14 study1, for early breast cancer patient with pathology result of ER +ve & Node –ve, 85% of women were disease free with tamoxifen alone. Is she belong to 85% ? How can we know who are these women? Fisher et al. N Engl J Med 1989;320(8):479-84
Chemotherapy + Hormonal Therapy for her ? • Base on NSABP B20 study, by treating 100 women (early breast cancer ER + LN-ve ) with chemotherapy and hormonal therapy only 4 would derive a benefit from chemotherapy treatment and 85 would have done well with hormonal therapy alone. How can we determine which women will benefit from chemotherapy, Which 85% will do fine without it? Fisher et al. J Natl Cancer Inst 1997;89:1673-82
Are there any genomic tools that help to determine those patients with highest risks of recurrence and thus benefit most from chemotherapy?
The 21st Century: genomic era Toward personalized medicine • As new technologies emerge in the 21st century , a number of gene expression signatures have been developed . They can give us information on molecular characteristics of cancer . • to assess an individual’s risk of recurrence • to provide personalized treatment plan • to identify those patients who benefit most from chemotherapy and those who will only benefit from endocrine therapy can be spare the adverse effects of chemotherapy.
Multi-gene assays for Breast Cancer Gene-Expression Signatures in Breast Cancer Molecular Origins of Cancer Christos Sotiriou et al. The New England Journal of Medicine. Boston: Feb 19, 2009. Vol. 360, Iss. 8; pg. 790 • Two commercially available assays that use in the clinical setting have been developed. • The 21-gene recurrence score ( Oncotype DX®; Genomic Health, Red-wood City, Calif. ) and • The Amsterdam 70-gene signature ( Mammaprint®; Agendia, Amsterdam, The Netherlands )
The 21-gene recurrence score (Oncotype DX®) Oncotype DX Breast Cancer Test Evaluates 21 Genes16 Cancer-Related and 5 Reference Genes From 3 Studies Estrogen Proliferation HER2 Invasion Others Reference Beta-actin GAPDH RPLPO GUS TFRC GRB7 HER2 Stromelysin 3 Cathepsin L2 CD68 ER PR Bcl2 SCUBE2 Ki-67 STK15 Survivin Cyclin B1 MYBL2 GSTM1 BAG1 It is an RT-PCR assay (reverse-transcriptase-polymerase-chain-reaction ) that measures the expression of 21 genes—16 cancer-related genes and 5 reference genes—in RNA extracted from paraffin-embedded tumor tissue Paik S, et al. N Engl J Med. 2004;351:2817.
Levels of Gene Expression Determine Recurrence Score Higher expression levels of “favorable” genes = ↓ RS Higher expression levels of “unfavorable” genes = ↑ RS Cutoff points chosen based on Results of NSABP trial B-20 A risk score is calculated from 0 -100 Sparano, J & Paik, S. JCO, 2008.
The 21-gene recurrence score (Oncotype DX) Validation Study No distant recurrence (low risk) = 93.2% No distant recurrence (high risk) = 69.5% p<0.001 1.NSABP B14 : National Surgical Adjuvant Breast and Bowel Project clinical trial B-14 2.Paik S, et al. N Engl J Med. 2004;351:2817-2826 • RS was significantly correlated with relapse free interval & OS (p<0.001) • Rate of distant recurrence at 10 years: • Low risk – 6.8% • Intermediate risk – 14.3% • High risk – 30.5%
Oncotype DX Assay ® is the gene expression analysis give information on molecular characteristics of cancer (gene signature), which is able to allow design of tailor made treatment plans for breast cancer patients. The Oncotype DX® Recurrence Score ® is a Continuous Predictor of Recurrence Risk of breast cancer. • Lower RSs • Lower likelihood of recurrence • Greater magnitude of TAM benefit • Likely minimal, if any, chemotherapy benefit • Higher RSs • Greater likelihood of recurrence • Lower magnitude of TAM benefit • Likely clear chemotherapy benefit 1) Paik et al NEJM 2004, 2) Habel et al Breast Cancer Research 2006 3) Paik et al JCO 2006, 4) Gianni et al JCO 2005
What is 70-gene profile (Mammaprint )? Web Source: Agendia
70-gene profile (MammaPrint) Web Source :Agendia • It is DNA microarray assay and requires a fresh / frozen sample of tissue that is composed of a minimum of 30% malignant cells. • It measures the expression of 70 genes and calculates a prognostic score that categorizes patients into • “good” or • “poor” risk groups. 1.van’t Veer LJ, et al. Nature 2002;415:530-6.
70-gene profile (MammaPrint) • Mammaprint has been validated to be prognostic in both node-negative and node- positive patient1and to be superior to adjuvant! Online in predicting distant recurrence 2 . 94.5% 85.2% 50.6% 54.6% 1.Van de Vijver et al. NEJM, 2002 2. Buyse, M. ed al. J of NCI, 2006 NB1, patient ages <53 with T1-2, LN-/+ primary breast cancer NB2. patient with age<60, T1-2, LN-
Prospective Validation of mammaprint : The MINDACT Trial There is an ongoing prospective randomized European Study, the Microarray in Node- Negative Disease may Avoid Chemotherapy ( MINDACT ) to study the ability of the 70 gene profile to predict clinical benefit from chemotherapy
Readiness of multi-gene assays for clinical use? 1.Harris L,et al. J Clin Oncol. 2007;25(33):5287-312. 2.NCCN Clinical Practice Guidelines in Oncology™ Breast Cancer, (Version 1.2011) Oncotype DX® has been endorsed by ASCO1 and NCCN2 guidelines to assist clinicians in making decisions about treatment. Mammaprint® has been cleared by the FDA for clinical use . In St. Gallen Consensus 2009 , the panel agreed that validated multi-gene tests, if readily available, could assist in deciding whether to add chemotherapy in cases where its use was uncertain after conventional markers.
Case Study Revisited Madam Choi, 59/F, Excellent Good Past Health Has newly Dx CA Left breast ,presented with left breast mass , Confirmed by imaging (MMG/ USG) and histology (Core Biopsy) WLE + Sentinel lymph node biopsy Pathology: Primary tumor - 2.2cm ,Grade 2, invasive ductal carcinoma, clear resection margins ER 300(+++), PR 300(+++), cerb2 –ve. No lymphovascular invasion Sentinel lymph nodes – 0/2 Stage IIA (pT2 N0M0) Base on the St. Gallen Criteria, she was classified to have intermediate risks. So she decided for further gene expression signatures test , Oncotype Dx
Oncotype DX® Recurrence Score® result RESULTS 0 Recurrence Score = CLINICAL EXPERIENCE Patients with a Recurrence Score of 0 in clinical validation study had an Average Rate of Distant Recurrence at 10 years of 3% .
Oncotype DX® Recurrence Score® result RESULTS 0 Recurrence Score = CLINICAL EXPERIENCE Patients with a Recurrence Score of 0 in clinical validation study had an Average Rate of Distant Recurrence at 10 years of 3% . Her Recurrence score is 0 and her average rate of distant recurrence at 10 years is 3%. Lower likelihood of recurrence Greater magnitude of tamoxifen benefit Likely minimal, if any, chemotherapy benefit
Case study revisited She was recommended RT + Tamoxifen/ Aromatase Inhibitor after joint discussion with oncologist and surgeon. She finally decided for RT + Tamoxifen alone as postoperative systemic adjuvant treatment. She can avoid the S/E of chemotherapy.
Conclusion Systemic adjuvant treatment improves survival for operable breast cancer patient by tackling the micro-metastasis . Decision for adjuvant treatment are made after balancing the risks and benefits. Gene expression signatures (OncotypeDx and Mammaprint) allow us to determine individual’s risk of recurrence and to aid selection of optimal therapy for individual patients. There are ongoing prospective randomized trial for the gene expression signatures ( TAILORx and MINDACT).
Table 3. Chemoendocrine therapy in patients with ER-positive, HER2-negative disease
Trastuzumab ( Herceptin) • Trastuzumab, a monoclonal antibody • was successfully developed to attack the cell • Surface receptors of Her2/Neu oncogene found in breast cancer cells
Prognostic significance – HER2/neu • 20% of breast cancer patients have HER2/neu gene amplification • Gene amplification ® cytoplasm glucoprotein overexpression • HER2 amplification or overexpression has been associated with higher tumour grade, negative ER status, higher tumour proliferation (e.g. Ki-67); and therefore poor prognosis • IHC (expression) vs. FISH (gene amplification)