Download
1 / 1
10 likes | 179 Vues
Telephone-Based Assessment and Management of Depression in Primary Care Clinics: The Behavioral Health Laboratory. J. Ross 1,2 , E. Ingram 1 , C. Beswick 1 , J. Murphy 1,2, , V. Kane 1 , I. R Katz 1,2 , D. W. Oslin 1,2.

E N D
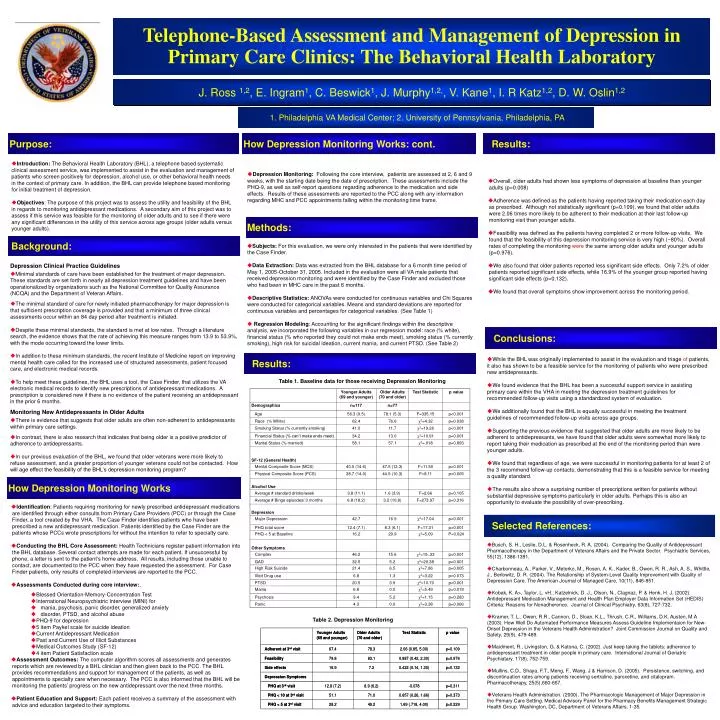
Telephone-Based Assessment and Management of Depression in Primary Care Clinics:The Behavioral Health Laboratory J. Ross 1,2, E. Ingram1, C. Beswick1, J. Murphy1,2,, V. Kane1, I. R Katz1,2, D. W. Oslin1,2 1. Philadelphia VA Medical Center; 2. University of Pennsylvania, Philadelphia, PA Purpose: How Depression Monitoring Works: cont. Results: Introduction: The Behavioral Health Laboratory (BHL), a telephone based systematic clinical assessment service, was implemented to assist in the evaluation and management of patients who screen positively for depression, alcohol use, or other behavioral health needs in the context of primary care. In addition, the BHL can provide telephone based monitoring for initial treatment of depression. Objectives: The purpose of this project was to assess the utility and feasibility of the BHL in regards to monitoring antidepressant medications. A secondary aim of this project was to assess if this service was feasible for the monitoring of older adults and to see if there were any significant differences in the utility of this service across age groups (older adults versus younger adults). Depression Monitoring: Following the core interview, patients are assessed at 2, 6 and 9 weeks, with the starting date being the date of prescription. These assessments include the PHQ-9, as well as self-report questions regarding adherence to the medication and side effects. Results of these assessments are reported to the PCC along with any information regarding MHC and PCC appointments falling within the monitoring time frame. Overall, older adults had shown less symptoms of depression at baseline than younger adults (p=0.008) Adherence was defined as the patients having reported taking their medication each day as prescribed. Although not statistically significant (p=0.109), we found that older adults were 2.06 times more likely to be adherent to their medication at their last follow-up monitoring visit than younger adults. Feasibility was defined as the patients having completed 2 or more follow-up visits. We found that the feasibility of this depression monitoring service is very high (~80%). Overall rates of completing the monitoring were the same among older adults and younger adults (p=0.976). We also found that older patients reported less significant side effects. Only 7.2% of older patients reported significant side effects, while 16.9% of the younger group reported having significant side effects (p=0.132). We found that overall symptoms show improvement across the monitoring period. Methods: Background: Subjects: For this evaluation, we were only interested in the patients that were identified by the Case Finder. Data Extraction: Data was extracted from the BHL database for a 6 month time period of May 1, 2005-October 31, 2005. Included in the evaluation were all VA male patients that received depression monitoring and were identified by the Case Finder and excluded those who had been in MHC care in the past 6 months. Descriptive Statistics: ANOVAs were conducted for continuous variables and Chi Squares were conducted for categorical variables. Means and standard deviations are reported for continuous variables and percentages for categorical variables. (See Table 1) Regression Modeling: Accounting for the significant findings within the descriptive analysis, we incorporated the following variables in our regression model: race (% white), financial status (% who reported they could not make ends meet), smoking status (% currently smoking), high risk for suicidal ideation, current mania, and current PTSD. (See Table 2) Depression Clinical Practice Guidelines Minimal standards of care have been established for the treatment of major depression. These standards are set forth in nearly all depression treatment guidelines and have been operationalized by organizations such as the National Committee for Quality Assurance (NCQA) and the Department of Veteran Affairs. The minimal standard of care for newly initiated pharmacotherapy for major depression is that sufficient prescription coverage is provided and that a minimum of three clinical assessments occur within an 84 day period after treatment is initiated. Despite these minimal standards, the standard is met at low rates. Through a literature search, the evidence shows that the rate of achieving this measure ranges from 13.9 to 53.9%, with the mode occurring toward the lower limits. In addition to these minimum standards, the recent Institute of Medicine report on improving mental health care called for the increased use of structured assessments, patient focused care, and electronic medical records. To help meet these guidelines, the BHL uses a tool, the Case Finder, that utilizes the VA electronic medical records to identify new prescriptions of antidepressant medications. A prescription is considered new if there is no evidence of the patient receiving an antidepressant in the prior 6 months. Monitoring New Antidepressants in Older Adults There is evidence that suggests that older adults are often non-adherent to antidepressants within primary care settings. In contrast, there is also research that indicates that being older is a positive predictor of adherence to antidepressants. In our previous evaluation of the BHL, we found that older veterans were more likely to refuse assessment, and a greater proportion of younger veterans could not be contacted. How will age effect the feasibility of the BHL’s depression monitoring program? Conclusions: Results: While the BHL was originally implemented to assist in the evaluation and triage of patients, it also has shown to be a feasible service for the monitoring of patients who were prescribed new antidepressants. We found evidence that the BHL has been a successful support service in assisting primary care within the VHA in meeting the depression treatment guidelines for recommended follow-up visits using a standardized system of evaluation. We additionally found that the BHL is equally successful in meeting the treatment guidelines of recommended follow-up visits across age groups. Supporting the previous evidence that suggested that older adults are more likely to be adherent to antidepressants, we have found that older adults were somewhat more likely to report taking their medication as prescribed at the end of the monitoring period than were younger adults. We found that regardless of age, we were successful in monitoring patients for at least 2 of the 3 recommend follow-up contacts, demonstrating that this is a feasible service for meeting a quality standard. The results also show a surprising number of prescriptions written for patients without substantial depressive symptoms particularly in older adults. Perhaps this is also an opportunity to evaluate the possibility of over-prescribing. Table 1. Baseline data for those receiving Depression Monitoring How Depression Monitoring Works • Identification: Patients requiring monitoring for newly prescribed antidepressant medications are identified through either consults from Primary Care Providers (PCC) or through the Case Finder, a tool created by the VHA. The Case Finder identifies patients who have been prescribed a new antidepressant medication. Patients identified by the Case Finder are the patients whose PCCs wrote prescriptions for without the intention to refer to specialty care. • Conducting the BHL Core Assessment: Health Technicians register patient information into the BHL database. Several contact attempts are made for each patient. If unsuccessful by phone, a letter is sent to the patient’s home address. All results, including those unable to contact, are documented to the PCC when they have requested the assessment. For Case Finder patients, only results of completed interviews are reported to the PCC. • Assessments Conducted during core interview:. • Blessed Orientation-Memory-Concentration Test • International Neuropsychiatric Interview (MINI) for • mania, psychosis, panic disorder, generalized anxiety • disorder, PTSD, and alcohol abuse • PHQ-9 for depression • 5 item Paykel scale for suicide ideation • Current Antidepressant Medication • Past and Current Use of Illicit Substances • Medical Outcomes Study (SF-12) • 4 item Patient Satisfaction scale • Assessment Outcomes: The computer algorithm scores all assessments and generates reports which are reviewed by a BHL clinician and then given back to the PCC. The BHL provides recommendations and support for management of the patients, as well as appointments to specialty care when necessary. The PCC is also informed that the BHL will be monitoring the patients’ progress on the new antidepressant over the next three months. • Patient Education and Support: Each patient receives a summary of the assessment with advice and education targeted to their symptoms. Selected References: Busch, S. H., Leslie, D.L. & Rosenheck, R. A. (2004). Comparing the Quality of Antidepressant Pharmacotherapy in the Department of Veterans Affairs and the Private Sector. Psychiatric Services, 55(12), 1386-1391. Charbonneau, A., Parker, V., Meterko, M., Rosen, A. K., Kader, B., Owen, R. R., Ash, A. S., Whittle, J., Berlowitz, D. R. (2004). The Relationship of System-Level Quality Improvement with Quality of Depression Care. The American Journal of Managed Care, 10(11), 846-851. Kobak, K. A>, Taylor, L. vH., Katzelnick, D. J., Olson, N., Clagnaz, P. & Henk, H. J. (2002). Antidepressant Medication Management and Health Plan Employer Data Information Set (HEDIS) Criteria: Reasons for Nonadherence. Journal of Clinical Psychiatry, 63(8), 727-732. Kramer, T. L., Owen, R.R., Cannon, D., Sloan, K.L., Thrush, C.R., Williams, D.K. Austen, M.A (2003). How Well Do Automated Performance Measures Assess Guideline Implementaion for New-Onset Depression in the Veterans Health Administration? Joint Commission Journal on Quality and Safety, 29(9), 479-489. Maidment, R., Livingston, G. & Katona, C. (2002). Just keep taking the tablets: adherence to antidepressant treatment in older people in primary care. International Journal of Geriatric Psychiatary, 17(8), 752-759. Mullins, C.D., Shaya, F.T., Meng, F., Wang, J & Harrison, D. (2005). Persistence, switching, and discontinuation rates among patients receiving sertraline, paroxetine, and citalopram. Pharmacotherapy, 25(5),660-667. Veterans Health Administration. (2000). The Pharmacologic Management of Major Depression in the Primary Care Setting. Medical Advisory Panel for the Pharmacy Benefits Management Strategic Health Group. Washington, DC, Department of Veterans Affairs, 1-35. Table 2. Depression Monitoring