Download
1 / 34
360 likes | 401 Vues
Beta-Lactam Antibiotics & Other Cell Wall Synthesis Inhibitors. Haitham Mahmood Alwali Ph.D. Pharmacology & Therapeutics College of Medicine/Al- Nahrain University. Penicillins and cephalosporins are the major antibiotics that inhibit bacterial cell wall synthesis.

E N D
Beta-Lactam Antibiotics& Other Cell WallSynthesis Inhibitors HaithamMahmoodAlwali Ph.D. Pharmacology & Therapeutics College of Medicine/Al-Nahrain University Haitham Alwali
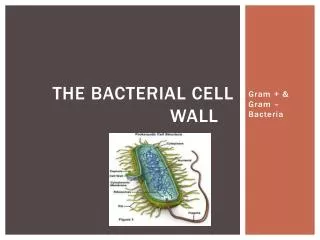
Penicillins and cephalosporins are the major antibiotics that inhibit bacterial cell wall synthesis. They are called beta-lactams because of the unusual 4-member ring that is common to all their members. The beta-lactams include some of the most effective, widely used, and well-tolerated agents available for the treatment of microbial infections. Haitham Alwali
Alexander Fleming Haitham Alwali
PENICILLINS • Classification All penicillins are derivatives of 6-aminopenicillanic acid and contain a beta-lactam ring structure that is essential for antibacterial activity. Penicillin subclasses have additional chemical substituents that confer differences in antimicrobial activity, susceptibility to acid and enzymatic hydrolysis, and biodisposition. Haitham Alwali
Pharmacokinetics • Routes of administration: 1-The combination of ampicillin with sulbactam, ticarcillin with clavulanic acid, and piperacillinwith tazobactam, and the antistaphylococcalpenicillinsnafcillin and oxacillin must be administered intravenously (IV) or intramuscularly (IM). Penicillin V, amoxicillin, and dicloxacillin are available only as oral preparations. Others are effective by the oral, IV, or IM routes Haitham Alwali
2- Depot forms: Procaine penicillin G and benzathine penicillin G are administered IM and serve as depot forms. They are slowly absorbed into the circulation and persist at low levels over a long time period. b. Absorption: Most of the penicillins are incompletely absorbed after oral administration, and they reach the intestine in sufficient amounts to affect the composition of the intestinal flora. Food decreases the absorption of all the penicillinase-resistant penicillins because as gastric emptying time increases, the drugs are destroyed by stomach acid. Therefore, they should be taken on an empty stomach. Haitham Alwali
C- Distribution:. All the penicillins distribute well & cross the placental barrier, but none have been shown to have teratogenic effects. However, penetration into bone or (CSF) is insufficient for therapy unless these sites are inflamed. D-Excretion: The primary route of excretion is by glomerular filtration. Patients with impaired renal function must have dosage regimens adjusted. Nafcillin and oxacillinare metabolized in the liver Probenecidinhibits the secretion of penicillins by competing for active tubular secretion via the organic acid transporter and, thus, can increase blood levels. Haitham Alwali
Mechanisms of Action and Resistance Beta-lactam antibiotics are bactericidal drugs. They act to inhibit cell wall synthesis by the following steps: • Binding of the drug to specific enzymes (penicillin-binding proteins [PBPs]) located in the bacterial cytoplasmic membrane; (2) inhibition of the transpeptidation reaction that cross-links the linear peptidoglycan chain constituents of the cell wall; and (3) activation of autolytic enzymes that cause lesions in the bacterial cell wall. Haitham Alwali
mechanism of bacterial resistance: • The formation of beta-lactamases (penicillinases) by most staphylococci and many gram-negative organisms. • Inhibitors of these bacterial enzymes (eg, clavulanic acid, sulbactam, tazobactam) are often used in combination with penicillins to prevent their inactivation. • Structural change in target PBPs is responsible for methicillin resistance in staphylococci and for resistance to penicillin G in pneumococci (eg, PRSP, penicillin resistant Streptococcus pneumoniae) and enterococci. • In some gram-negative rods (eg, Pseudomonas aeruginosa), changes in the porin structures in the outer cell wall membrane may contribute to resistance by impeding access of penicillinsto PBPs. Haitham Alwali
Clinical Uses 1. Narrow-spectrum penicillinase-susceptible agents— Penicillin G is the prototype of a subclass of penicillins. Clinical uses include therapy of infections caused by common streptococci, meningococci, gram-positive bacilli, and spirochetes. Many strains of pneumococci (penicillin-resistant S. pneumoniae [PRSP] strains). Staphylococcus aureusand Neisseria gonorrhoeaeare resistant via production of beta-lactamases. penicillin G remains the drug of choice for syphilis. Activity against enterococci is enhanced by coadministration of aminoglycosides. Penicillin V is an oral drug used mainly in oropharyngeal infections. Haitham Alwali
2. Very-narrow-spectrum penicillinase-resistant drugs— This subclass of penicillins includes methicillin (the prototype,but rarely used owing to its nephrotoxic potential), nafcillin,and oxacillin. Their primary use is in the treatment of known or suspected staphylococcal infections. Methicillin-resistant (MR)staphylococci(S.aureus[MRSA] and S.epidermidis[MRSE]) areresistant to all penicillins and are often resistant to multiple antimicrobial drugs. Haitham Alwali
3. Wider-spectrum penicillinase-susceptible drugs a. Ampicillin and amoxicillin—has a wider spectrum of antibacterial activitythan penicillin G. Their clinical uses include indications similar to penicillin G as wellas infections resulting from enterococci, Listeria monocytogenes, Escherichia coli, Proteus mirabilis, Haemophilusinfluenzae, andMoraxella catarrhalis, although resistant strains occur. Whenused in combination with inhibitors of penicillinases (eg, clavulanicacid), their antibacterial activity is often enhanced. Inenterococcaland listerial infections, ampicillin is synergistic with aminoglycosides. Haitham Alwali
b. Piperacillin and ticarcillin— These drugs have activityagainst several gram-negative rods, including Pseudomonas,Enterobacter, and in some cases Klebsiella species. Most drugsin this subgroup have synergistic actions with aminoglycosidesagainst such organisms. Piperacillin and ticarcillin are susceptible to penicillinases and are often used in combination with penicillinaseinhibitors (eg, tazobactam and clavulanic acid) to enhancetheir activity. Haitham Alwali
E. Toxicity 1. Allergy—Allergic reactions include urticaria, severe pruritus, fever, joint swelling, hemolytic anemia, nephritis, and anaphylaxis. Methicillin causes interstitial nephritis, and nafcillin is associated with neutropenia. Complete cross-allergenicity between different penicillins should be assumed. 2. Gastrointestinal disturbances— Nausea and diarrhea may occur with oral penicillins, especially with ampicillin. Gastrointestinal upsets may be caused by direct irritation or by overgrowth of gram-positive organisms or yeasts. Haitham Alwali
CEPHALOSPORINS The cephalosporinsare β-lactam antibiotics that are closely related both structurally and functionally to the penicillins. Most cephalosporinsare produced semisynthetically by the chemical attachment of side chains to 7-aminocephalosporanic acid. Cephalosporins have the same mode of action as penicillins, and they are affected by the same resistance mechanisms. However, they tend to be more resistant than the penicillins to certain β-lactamases. Haitham Alwali
Pharmacokinetics Several cephalosporins are available for oral use, but most are administered parenterally. Cephalosporinswith side chains may undergo hepatic metabolism, but the major elimination mechanism for drugs in this class is renal excretion via active tubular secretion. Cefoperazoneand ceftriaxone are excreted mainly in the bile. Most first- and second-generation cephalosporinsdo not enter the cerebrospinal fluid even when the meninges are inflamed. Haitham Alwali
Mechanisms of Action and Resistance Cephalosporins bind to PBPs on bacterial cell membranes to inhibit bacterial cell wall synthesis by mechanisms similar to those of the penicillins. Cephalosporins are bactericidal against susceptible organisms. Cephalosporins less susceptible to penicillinases produced by staphylococci, but many bacteria are resistant through the production of other betalactamasesthat can inactivate cephalosporins. Resistance can also result from decreases in membrane permeability to cephalosporins and from changes in PBPs. Methicillin-resistant staphylococci are also resistant to cephalosporins. Haitham Alwali
Clinical Uses • First-generation drugs—Cefazolin(parenteral) and cephalexin (oral) are examples of this subgroup. They are active against gram-positive cocci, including staphylococci and common streptococci. Many strains of E coli and K pneumoniaeare also sensitive. • Clinical uses include treatment of infections caused by these organisms and surgical prophylaxis in selected conditions. Haitham Alwali
2. Second-generation have slightly less activity against gram-positive organisms than the first-generation drugs but have an extended gram-negative coverage. Marked differences in activity occur among the drugs in this subgroup. Examples of clinical uses include infections caused by the anaerobe Bacteroides fragilis (cefotetan, cefoxitin) and sinus, ear, and respiratory infections caused by H influenzae or M catarrhalis (cefamandole, cefuroxime, cefaclor). Haitham Alwali
3. Third-generation drugs: (eg, ceftazidime, cefoperazone, cefotaxime) include increased activity against gram-negative organisms resistant to other beta-lactam drugs and ability to penetrate the blood-brain barrier (except cefoperazone and cefixime). • Most are active against Providencia, Serratiamarcescens, and beta-lactamase producing strains of H influenzae and Neisseria • Ceftriaxone and cefotaximeare currently the most active cephalosporins against penicillin-resistant pneumococci (PRSP strains) • Also have activity against Pseudomonas (cefoperazone, ceftazidime) and B fragilis(ceftizoxime) • Ceftriaxone (parenteral) and cefixime (oral), currently drugs of choice in gonorrhea. Haitham Alwali
4. Fourth-generation drugs— • Cefepimeis more resistant to beta-lactamases produced by gram-negative organisms, including Enterobacter, Haemophilus, Neisseria, and some penicillin resistant pneumococci. • Cefepimecombines the gram-positive activity of first-generation agents with the wider gram-negative spectrum of third-generation cephalosporins. • Ceftaroline has activity in infections caused by methicillin-resistant staphylococci. Haitham Alwali
Toxicity 1. Allergy—Cephalosporins cause a range of allergic reactions from skin rashes to anaphylactic shock. These reactions occur less frequently with cephalosporinsthan with penicillins. Complete cross-hypersensitivity between different cephalosporins should be assumed. Cross-reactivity between penicillins and cephalosporins is incomplete (5–10%). 2- Cephalosporinsmay cause pain at intramuscular injection sites and phlebitis after I.V administration. They may increase the nephrotoxicity of aminoglycosides when the two are administered together. Haitham Alwali
OTHER BETA-LACTAM DRUGS: A. Aztreonam • Aztreonamis a monobactam that is resistant to beta-lactamases produced by certain gram-negative rods, including Klebsiella, Pseudomonas, and Serratia. The drug has no activity against gram positive bacteria or anaerobes. • Aztreonam is administered intravenously and is eliminated via renal tubular secretion. Its half-life is prolonged in renal failure. • Adverse effects include gastrointestinal upset with possible superinfection, vertigo and headache, and rarely hepatotoxicity. Haitham Alwali
B. Imipenem, Doripenem, Meropenem, and Ertapenem: • These drugs are carbapenems (chemically different from penicillinsbut retaining the beta-lactam ring structure) • They have wide activity against gram-positive cocci (including some penicillin-resistant pneumococci), gram-negative rods, and anaerobes. • For pseudomonal infections, they are often used in combination with an aminoglycoside. • MRSA strains of staphylococci are resistant. Haitham Alwali
Imipenem is rapidly inactivated by renal dehydropeptidase-Iand is administered in fixed combination with cilastatin, an inhibitor of this enzyme. Cilastatin increases the plasma half life of imipenem and inhibits the formation of potentially nephrotoxic metabolite. • Adverse effects of imipenem-cilastatin include gastrointestinal distress, skin rash, and, at very high plasma levels, CNS toxicity (confusion, encephalopathy, seizures). • There is partial cross allergenicity with the penicillins. Haitham Alwali
C. Beta-Lactamase Inhibitors Clavulanic acid, sulbactam, and tazobactam are used in fixed combinations with certain hydrolyzablepenicillins. • They are most active against plasmid-encoded beta-lactamases such as those produced by gonococci, streptococci, E coli, and H influenzae. • They are not good inhibitors of inducible chromosomal beta-lactamases formed by Enterobacter, Pseudomonas, and Serratia. Haitham Alwali
OTHER CELL WALL OR MEMBRANE-ACTIVE AGENTS: A. Vancomycin • Vancomycinis a bactericidal glycoprotein that binds to the d-Ala-d-Alaterminal of the nascent peptidoglycan pentapeptide side chain and inhibits transglycosylation. This action prevents elongation of the peptidoglycan chain and interferes with crosslinking. • Resistance in strains of enterocci (vancomycin-resistant enterococci [VRE]) and staphylococci (vancomycin-resistant S aureus[VRSA]) involves a decreased affinity of vancomycinfor the binding site Haitham Alwali
Vancomycin has a narrow spectrum of activity and is used for serious infections caused by drug-resistant gram-positive organisms, including methicillin-resistant staphylococci (MRSA) and in combination with ceftriaxone for treatment of (PRSP). Vancomycin is for treatment of infections caused by Clostridium difficile. • Toxic effects of vancomycin include chills, fever, phlebitis, ototoxicity, and nephrotoxicity. Rapid intravenous infusion may cause diffuse flushing (“red man syndrome”) from histamine release. Haitham Alwali
B. Fosfomycin Fosfomycin is an antimetabolite inhibitor of cytosolic enolpyruvate transferase. This action prevents the formation of N-acetylmuramic acid, an essential precursor molecule for peptidoglycan chain formation. Fosfomycin is excreted by the kidney, with urinary levels exceeding the minimal inhibitory concentrations (MICs) for many urinary tract pathogens. Haitham Alwali
C. Bacitracin Bacitracin is a peptide antibiotic that interferes with a late stage in cell wall synthesis in gram-positive organisms. Because of its marked nephrotoxicity, the drug is limited to topical use. E. Daptomycin Daptomycinis a novel cyclic lipopeptide with spectrum similar to vancomycin but active against vancomycin-resistant strains of enterococci and staphylococci. The drug is eliminated via the kidney. Creatine phosphokinase should be monitored since daptomycin may cause myopathy. Haitham Alwali