Download
1 / 25
280 likes | 1.16k Vues
Multimodality Treatment of Mesenteric Desmoid Tumors. Brigham and Women’s Hospital Dana-Farber Cancer Institute Harvard Medical School CTOS Annual Meeting London November 13, 2008.

E N D
Multimodality Treatment of Mesenteric Desmoid Tumors Brigham and Women’s Hospital Dana-Farber Cancer Institute Harvard Medical School CTOS Annual Meeting London November 13, 2008 Monica M. Bertagnolli, Jeffrey A. Morgan, Christopher D.M. Fletcher, Chandrajit P. Raut, Palma Dileo, Ritu R. Gill, George D. Demetri and Suzanne George
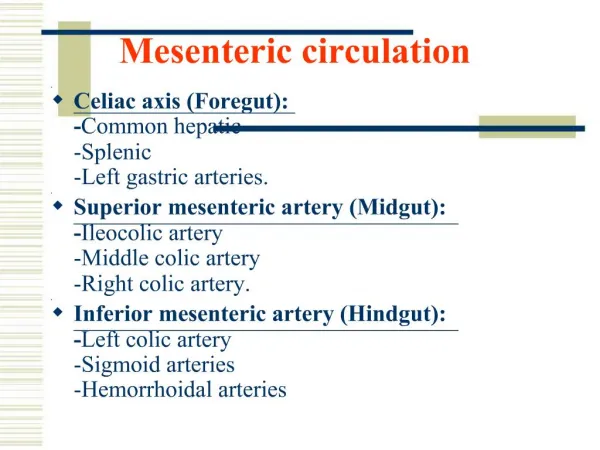
Desmoid tumors Clonal proliferation of fibroblasts with an abundant collagen matrix Occur in 10-20% of patients with Familial Polyposis mesentery 50% abdominal wall/trunk 48% extremities 2% multifocal 40% Sporadic tumors are rare (600-1200 per year in the US) extremity 60% abdominal wall/trunk 35% mesentery 5%
Mesenteric Desmoid tumors • Wide range of clinical behavior • Life threatening due to impact on small bowel and mesenteric blood supply • Surgery can be complex due to location • Radiation may be difficult due to toxicity associated with this anatomic site
CT Characteristics Infiltrative Localized
Methods • Single institution retrospective review • Consecutive series of patients with desmoid tumors of the intestinal mesentery, 2001-2005 • Patients were seen by both surgical and medical oncology • Reviewed treatment course and outcome
Methods • Tumor Characteristics at presentation to DFCI/BWH • Resectable vs Unresectable • all grossly visible tumor could be removed without sacrificing small bowel function • Progressing vs Stable • Infiltrative vs Localized
Treatment Strategy *1st line liposomal doxorubicin; 2nd line vinorelbine
Results: Patient Characteristics 52 pts 21 FAP (age 20-50, median 31) 31 sporadic (age 24-67, median 41) Prior NSAID, tamoxifen or both 60% Prior imatinib 12% Prior cytotoxic chemotherapy 8% Median Followup 50 months
Results: Disease Characteristics (n=52) • Localized disease 16 (31%) • Infiltrative disease 36 (69%) • Progressive disease 40 (78%) • Stable disease 12 (23%) • Resectable 36 (69%) • Unresectable 16 (31%)
Results: Extent of Surgery Significant postop complications 16% of pts – anastomotic leak, abcess, EC fistula, postop bleed All patients retained adequate small bowel function, no chronic TPN, no surgery associated deaths.
Results: Chemotherapy * by RECIST
Summary • Multidisciplinary assessment and treatment planning is effective in patients with mesenteric desmoid tumors • Tumor characteristics matter • No apparent detrimental effect of surgery with regard to disease control in carefully chosen patients • Chemotherapy can be effective in disease control • Observation is a reasonable approach in patients with non-progressing, asymptomatic disease
Limitations • Short followup • Relatively small number of patients • Variable natural history • Mesenteric location only - unknown application to desmoids of other body sites
Mesenteric desmoid tumors • Localized vs diffuse disease • Incidentally discovered during 12-22% of surgeries for FAP(Clark BrJSurg 1999, Hartley DC&R 2004) • 2nd leading cause of disease-related mortality in patients with FAP • 13% of FAP patients with desmoids in a series of 88 patients died within 5 years of diagnosis (Clark Br J Surg 1999)