Download

1 / 16
160 likes | 332 Vues
Medicare and the New Prescription Drug Benefit. Presented by Tricia Neuman, Sc.D. Vice President and Director, Medicare Policy Project The Henry J. Kaiser Family Foundation for KaiserEDU.org January 2004. Background and Context: Why Drug Coverage Matters. Exhibit 1.

E N D
Medicare and the New Prescription Drug Benefit Presented byTricia Neuman, Sc.D. Vice President and Director, Medicare Policy ProjectThe Henry J. Kaiser Family FoundationforKaiserEDU.org January 2004
Exhibit 1 Key Characteristics of the Medicare Population Percent of total Medicare population: Lack Drug Coverage (Full and Part Year) Low Income (<150% FPL or less than $13,965 in 2004) 1+ Functional Limitation Fair/Poor Health Rural Cognitive Impairment Under 65 Disabled Nursing Home/Assisted Living Resident SOURCE: Stuart and Briesacher, estimates based on 2000 MCBS; Medicare Current Beneficiary Survey, 1997-2002; Low-income estimate from Urban Institute based on March 2003 Current Population Survey.
Exhibit 2 Skipping Doses of Medication Among Chronically Ill Seniors With and Without Drug Coverage Percent of seniors in 8 states who skipped doses of medicine to make it last longer: SOURCE: Kaiser/Commonwealth/New England Medical Center 2001 Survey of Seniors in Eight States.
Exhibit 3 Medicare Beneficiaries’ Out-of-Pocket Prescription Drug Spending, 2000-2013 Average annual out-of-pocket drug costs among the Medicare population: Projected: * Without Medicare drug benefit. SOURCE: Actuarial Research Corporation analysis for The Kaiser Family Foundation, June 2003 and November 2004.
Exhibit 4 History of Medicare and Prescription Drugs, 1965-2003 1969: HEW Task Force on Prescription Drugs Report issued 1993: Clinton proposed a new Medicare Rx benefit as part of the Health Security Act 1965: Medicare enacted -no outpatient prescription drug coverage included 1989: Repeal of MCCA 2000: Clinton releases plan to provide drug coverage under a new Medicare Part D 1988: Passage of Medicare Catastrophic Coverage Act (MCCA)—drug benefit included 1965 1970 1975 1980 1985 1990 1995 2000 2003 2000: Republican-sponsored bill to create a Medicare drug benefit (H.R. 4680) passes the House of Representatives, 217-214 2002: Republican-sponsored bill to create a Medicare drug benefit. (H.R. 4954) passes the House of Representatives, 221-208; Several competing proposals for a Medicare drug benefit fail to pass the Senate 2003: Medicare Prescription Drug, Improvement, and Modernization Act signed into law by President Bush on December 8
Exhibit 5 Medicare Prescription Drug, Improvement, and Modernization Act of 2003 Phase 1: Medicare-Approved Drug Discount Card Program (June 2004 – December 31, 2005) • Cards provide discounts (not same as insurance) • New $600 credit in 2004 and 2005 for low-income beneficiaries who do not have Medicaid, with incomes below 135% poverty • 5.8 million beneficiaries currently enrolled (CMS, Dec 2004) • 1.4 million low-income beneficiaries receiving $600 subsidy (of ~7.2 million eligible) Phase 2: Medicare Prescription Drug Benefit (begins January 1, 2006) • Beneficiaries will have access to private plans that provide new prescription drug benefit under Medicare Estimated cost: $400 billion (CBO) to $553 billion (HHS) over 2004-2013 period
Exhibit 6 Medicare Prescription Drug Benefit (Part D) • Beginning in 2006, beneficiaries will have choice of: • Fee-for-service Medicare, with access to private plans offering prescription drug coverage only (PDPs) • Medicare Advantage plans covering Medicare benefits and prescription drugs (MA-PD plans • New plans will provide “standard” prescription drug benefit or its actuarial equivalent • Plans have flexibility (subject to certain constraints) to establish varying features: • Levels of cost-sharing requirements and coverage limits other than “standard” coverage • Lists of drugs to include on their formulary, and on which tier • Cost management tools • Premium and cost-sharing subsidies for beneficiaries with incomes up to 150% FPL ($13,965 for an individual in 2004) and modest assets up to $10,000
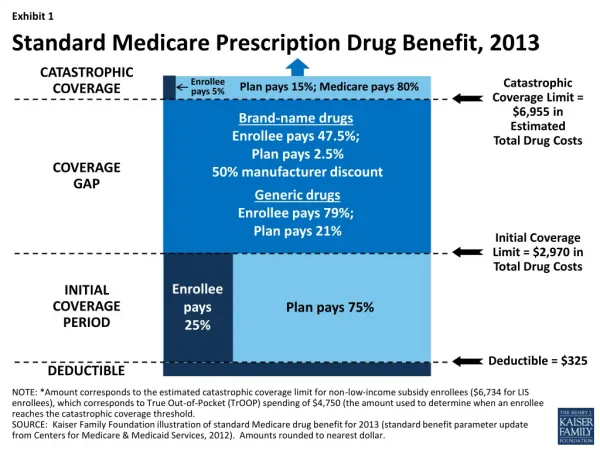
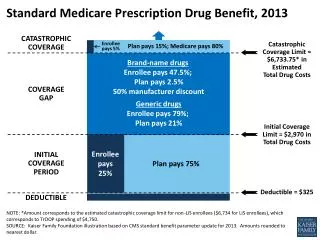
Exhibit 7 Standard Medicare Part D Drug Benefit, 2006 Beneficiary Out-of-PocketSpending Catastrophic Coverage Medicare Pays 95% 5% $5,100 in Total Drug Costs** $2,850 Gap: Beneficiary Pays 100% No Coverage $2,250 in Total Drug Costs* Partial Coverage up to Limit Medicare Pays 75% 25% $250 Deductible + ~$420 average annual premium *$2,250 in total spending is equivalent to $750 in out-of-pocket spending. **$5,100 in total spending is equivalent to $3,600 in out-of-pocket spending. SOURCE: Kaiser Family Foundation analysis of Medicare Prescription Drug, Improvement, and Modernization Act of 2003.
Exhibit 8 Provisions in the MMA for Low-Income Beneficiaries • Premium and cost-sharing subsidies, with most generous assistance provided to those with lowest incomes • 6.5 million Medicare beneficiaries eligible for full Medicaid benefits (“dual eligibles”) • Beneficiaries with incomes <135% FPL ($12,569/individual in 2004) and assets <$6,000/individual • Beneficiaries with incomes 135%-150% FPL ($12,569-$13,965/individual in 2004) and assets <$10,000/individual • Treatment of dual eligibles • Medicaid stops paying for prescription drugs after December 31, 2005 • Dual eligibles can enroll in Part D plans, or will be auto-enrolled, if necessary • Key questions: • Will “dual eligibles” transition from Medicaid to Medicare plans without falling through cracks? • Will “dual eligibles” be able to get needed medications under new Medicare plans?
Exhibit 9 The MMA is Projected to Reduce Average Out-of-Pocket Spending but the Extent of the Reduction is Likely to Vary All Other Part D Participants(20.3 million) Part D Participants Who Receive Low-Income Subsidies(8.7 million) Average Change:- 37% SOURCE: Actuarial Research Corporation analysis for the Kaiser Family Foundation, November 2004.
Exhibit 10 Gap in Standard Part D Benefit in 2006 Could Leave Many Part D Participants Vulnerable to High Out-of-Pocket Spending 8.6 million 6.9 Million Part D Participants Reach the “Doughnut Hole”in 2006 10.5 million 3.0 million Total = 29 Million Part D Participants NOTE: Estimates exclude premiums and assume no supplementation of Part D coverage. SOURCE: Actuarial Research Corporation analysis for the Kaiser Family Foundation, November 2004.
Exhibit 11 Challenges for Beneficiaries • Learning about Part D • Comparing features of plans available within a region, including premiums, cost-sharing, formularies, and pharmacy networks • Learning about low-income subsidy programs and eligibility rules • Learning about the rules of enrollment, including premium penalty for delayed enrollment and annual plan lock-in • Enrolling in Part D • Choosing between traditional fee-for-service and a stand-alone PDP, or a Medicare Advantage plan that covers prescription drugs (where available) • Enrolling in low-income subsidy program, if eligible, at Social Security or state Medicaid office • Using the New Benefit • Tracking total and out-of-pocket drug spending • Coordinating Part D with other sources of drug coverage (state pharmacy assistance programs, employer coverage, etc.)
Exhibit 12 Decisions for Medicare Beneficiaries, 2006 Enroll in Part D Plan Medicare Advantage Traditional Medicare Part D Prescription Drug Plan No Part D coverage HMO (local) PPO (regional) Private Fee-for-Service Apply for Low-Income Subsidy Social Security Office Dual Eligibles Medicaid Office Meet Income and Asset Test? If yes, qualify for: Below 150% FPL: Subsidy for premium on sliding scale, $50 deductible, 15% coinsurance to $5,100 in Rx costs, $2/generic Rx, $5/brand name Rx after $5,100 Below 100% FPL: No premium or deductible, $1/generic Rx, $3/brand name Rx, pay nothing after $5,100 in Rx costs Below 135% FPL: Subsidy for premium, no deductible, $2/generic Rx, $5/brand name Rx, pay nothing after $5,100 in Rx costs
Exhibit 13 Conclusions • Implementation deadlines pose big challenge for CMS, plans, beneficiaries • Plan bids due in June, awarded September, plans announced Oct 15, 2005 • Low-income subsidy enrollment begins June 2005 • Initial enrollment period from Nov 15, 2005 to May 15, 2006 • Beneficiary education will be critical to ease confusion, help transition of dual eligibles to Part D, and inform plan choice • Medicare drug benefit projected to reduce out-of-pocket drug spending, especially for low-income, but many unknowns • Will new prescription drug-only plans emerge? • Will seniors sign up for Part D and low-income subsidies? • Will dual eligibles transition from Medicaid to Medicare? • Will new drug plans cover needed medications? • Important to monitor beneficiaries’ access to needed medications and out-of-pocket prescription drug spending as new Medicare drug benefit is implemented.