Download
1 / 32
320 likes | 474 Vues
Child and Youth Mental Health Service Redesign Demonstration Projects. Information Session Thursday 4 September 2008. Housekeeping. Please check that your contact details are correct at the desk Structure of session: Background to the Mental Health Reform Strategy and Demonstration Projects

E N D
Child and Youth Mental Health Service Redesign Demonstration Projects Information Session Thursday 4 September 2008
Housekeeping • Please check that your contact details are correct at the desk • Structure of session: • Background to the Mental Health Reform Strategy and Demonstration Projects • The submission process • The selection process • The implementation process • Questions
Please note: • The information contained in this presentation aims to clarify key aspects of the submission brief in discussion with prospective lead agencies. The submission brief contains the complete description of all DHS requirements and therefore remains the primary source of information in relation to the demonstration projects. • In recognition of the competitive nature of this submission process, the DHS undertakes to use standards of probity and transparency normally associated with public tendering processes.
Project team • Bill MacDonald, Manager Child and Youth Mental Health Services, Operations Branch, Mental Health and Drugs Division, Department of Human Services (ph 03-9096 7971; email bill.macdonald@dhs.vic.gov.au). • Gilbert Van Hoeydonck, Project Leader, Child and Youth Mental Health Services, Operations Branch, Mental Health and Drugs Division, Department of Human Services (ph. 03-9096 7905; email gilbert.vanhoeydonck@dhs.vic.gov.au).
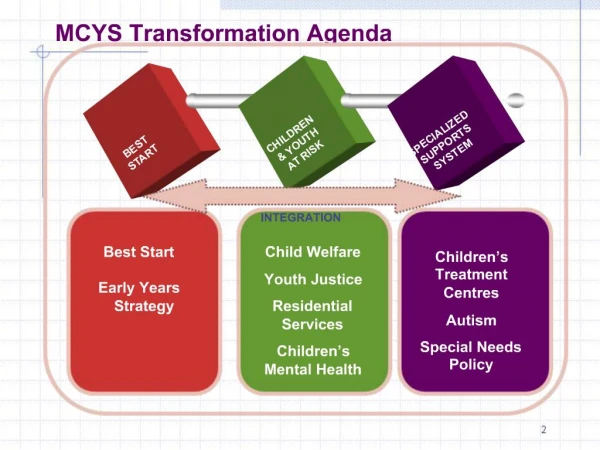
Mental health reform strategy • A whole-of-government reform initiative • May 2008 Green Paper: Because mental health matters • Final Reform Strategy paper to be completed by the end of 2008 • The finalised Strategy will provide the context for project activities
Focus areas for reform • Prevention • Early intervention • Access • Specialist care • Complex clients • Workforce • Partnerships
Strategic priorities • Priority focus on children, young people and families • Early in life • Early in illness • Early in episode • Focus Area 2 – Early Intervention • Other action areas relevant
Focus Area 2 – Early intervention • Strengthen capacity for early identification and intervention through universal services. • Provide earlier and age-appropriate treatment and support for children and young people with emerging or existing mental health problems and their families. • Deliver appropriate mental health support for particular groups of vulnerable young people. • Build stronger, more resilient families where there is risk related to mental health problems or a combined mental health and drug and alcohol problem.
Demonstration projects • Seeding mental health reform • Two four-year projects (2008-2012) • One rural, one metropolitan project • Need to develop or strengthen partnerships within and between services: • Submissions accepted only from multi-service consortia • Strong emphasis upon collaboration with primary care providers, education and other human service providers throughout the projects
Aim (part A section 2) • Reduce the prevalence of untreated mental health problems and disorders across the 0-25 age group within the designated catchment area by providing earlier recognition and timely responses to a larger number of children and young people with a broader range of mental health problems and disorders.
Seeding significant reform • The demonstration projects will critically re-examine: • who should receive services and from whom, • the timing of service engagement and support, • the type of interventions delivered, • the way that services are organised; and • the location of service outlets.
Scope of reform (2.2) • Remove barriers within and between services • Better age-appropriate integrated responses across clinical and PDRSS • New early intervention services for 0-12 and 12-25 years with primary care • Age-appropriate partnerships • Better respond to vulnerable young people including child protection and youth justice
Expected outcomes include (2.3 & 4): • Increased numbers being seen with a broader range of problems across the age range • Earlier and age-appropriate interventions • Services provided from familiar local settings that are easier to access and use • Broader range of treatment options • Improved continuity of care across service types and programs • Recovery-focused care, where clinical and non-clinical services work together to address whole-of-life circumstances
Initial priority areas • In the first instance, consortia will be required to focus on two priority areas in planning demonstration activity to ensure general system readiness to respond early: • Expanding assessment of and responsiveness to pre-school and primary school aged children who display early signs of social, emotional and behavioural problems. • Developing strategies to better engage adolescents and young adults 12-25 years with a broader range of moderate to severe mental health problems, including co-occurring drug and alcohol problems.
Potential strategies • Regional needs analysis and mapping and planning of services. • Use a clear project management and change management framework. • Build partnerships. • Target service gaps, areas of high need. • Foster integrated service provision while providing differentiated responses to the specific needs of the various age groups.
Service reform principles (2.4) • Outcome Focus • Reform agenda • Shared responsibility • Early intervention • Recovery orientation • Consumer-centred approach • Evidence based planning and practice
Involving consumers and carers • A consumer-centred approach is one of the service reform principles. • Reform needs to be planned with and for consumers, carers and families. • Adequate advocacy and participation mechanisms to be implemented for children, adolescents, young adults and their families.
Project catchment (2.6) • Sub-regional to regional • One or more PCP or AMHS catchments • Practical • Metro 100,000 to 200,000 • Rural 50,000 to 100,000 • Final catchment size to be agreed.
Project outputs and timelines (2.8) • Appointment of a project co-ordinator (Dec 2008) • Development of a work plan (end Dec 2008) • Development of a Reform Action Plan (June 2009) • Draft Plan March 2009 • Endorsed by Consortia/RD and MH&D Division • June 2008 • Implementation of the Reform Action Plan • Staged approach • Commence 1 July 2009 • Revision of the Reform Action Plan continues over time
Submission process (Part B -5) • Consortia to include, at a minimum: • CAMHS • Adult Mental Health Service • PDRSS • Primary Health entity • Use template provided (Part D – p.26) • CEO sign-off for each consortium organisation • Deadline is 4:30pm on 17 October 2008
Points to address in the submission (Part D – Part 2) • Provide an outline of: • the proposed project area including areas of high need • how the project would be planned and developed locally to work in this area • how a practical, workable, collaborative and cross sector approach could be developed in accord with the service reform principles • the services to be involved, the extent of service reform being envisaged and the outcomes that you are aiming for • the capacity of the consortium to achieve these reforms - including the readiness of the consortium, the capacity of the mental health services and partner agencies to deliver the outcomes. Address both project management and service reform aspects • how it would be implemented, managed and monitored in accord with the service specifications. • Address all other requirements of the submission brief!
Key Selection Criteria (part B – 6) • Understanding of mental health reform • Needs and outcome targets • Capacity • Readiness • Financial and technical • Staffing and employment
Submission and selection timelines • 22 Aug 2008: demonstration projects announced • 4 Sept 2008: information session at DHS • Sept/Oct 2008: establish consortium, develop submission, obtain CEO sign-off • 17 October 2008: closing date for submissions • Week commencing 27 Oct 2008: interviews • 7 Nov 2008: selection process completed; successful consortia announced, • November 2008: $150K one-off provided for project management
Selection process • DHS target dates are: • Shortlisting completed by 24 October. • Interview shortlisted consortia in the week commencing 27 October 2008. • Advise successful consortia by 7 November 2008. • Selection panel to comprise representatives from relevant departments and agencies
Funding (2.10) • The CAMHS or AMHS in the consortium is to be the fund holder. • Funding will flow through a variation to the existing Service Agreement between DHS and the health service: • $150K upon confirmation of successful consortium; • pro-rata funding for 2008-09 as required by local Reform Action Plan; and • full-year funding from 2009-10 through 2011-12 of up to $1.9M p.a. for the metropolitan project and up to $900K p.a. for the rural project.
Service development grants (2.11) • Consortia must submit in accord with requirements of the brief (0-25) • Selection criteria will be used • Consortia can highlight area for service development activity in submission • Successful project consortia will not be eligible • Work plan will be required
Executive Director Mental Health and Drugs Division Project Management Group Statewide Advisory Group Project Team Project Support: Communication Strategies Workforce Development Evaluation Tender Rural Regional Partnership Group Consortium 1 Metropolitan Regional Partnership Group Consortium 2 Project structures
Regional Partnership Group (2.12) • Chaired by the DHS Regional Director • Representation of relevant programs/ sectors • Advises on the Reform Action Plan • RD signs off the Reform Action Plan • Receives reports and provides advice during the implementation phase
Role of the lead agency/fund holder • Area Mental Health Service • Bring together a consortium – minimum core mandatory membership and submission signed off by CEOs • Lead collaborative planning process in the development of the Reform Action Plan • Maintain effective working relationships with the Regional Partnership Group • Work closely with the Mental Health and Drugs Division in the development and delivery of the projects • Actively monitor and report on activity, progress, outcomes • Account to the Mental Health and Drugs Division for project funds • Manage the project deliverables in accord with the project specifications and the mental health reform strategy.
Evaluation (4) • The Mental Health & Drugs Division will appoint an evaluation contractor • assist DHS and the consortia on data collection, benchmarking, monitoring and measuring outcomes • Assist consortia with regular monitoring and reporting on project progress • Provide an independent summative evaluation of the process and its outcomes by early 2012.
Workforce development • The Mental Health & Drugs Division will identify training needs in consultation with consortia and the Statewide Advisory Group. • Work with existing training providers to plan and roll out workforce development program to support reform directions. • Training needs of staff in demonstration projects as the initial priority.
Questions • All answers to the questions raised during this information session will be written up, emailed to registered participants and uploaded to the website of the Mental Health and Drugs Division of DHS at http://www.dhs.vic.gov.au/mhd/index.htm