Download

1 / 44
480 likes | 794 Vues
Joint Hospital Grand Round Management of Chronic Gastric Volvulus. Kenny K Y Yuen Tseung Kwan O Hospital 20th January, 2007. Clinical scenario History Predisposing factors Classifications Clinical presentations Investigations Treatment. Clinical Scenario. F/29

E N D
Joint Hospital Grand RoundManagement of Chronic Gastric Volvulus Kenny K Y Yuen Tseung Kwan O Hospital 20th January, 2007
Clinical scenario • History • Predisposing factors • Classifications • Clinical presentations • Investigations • Treatment
Clinical Scenario • F/29 • Intermittent epigastric pain for years • Cramping after heavy meal, relieved after vomiting • Weight loss 5 kg within 2-3 months Upper endoscopy • twisted stomach with difficulty in finding pylorus
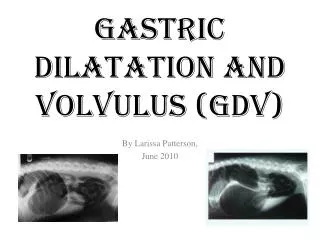
Clinical Scenario Erect AXR • Double air-fluid levels at LUQ Ba meal • Stomach rotated > 180o • Body rotates towards the R hemidiaphragm • Greater curve laying same level as the fundus • Organoaxial gastric volvulus • No hiatus hernia • No gastric outlet obstruction
Definition • Gastric volvulus is rotation of all or part of the stomach more than 180°, which may lead to a closed-loop obstruction and possible strangulation
1579 History of Gastric Volvulus Ambrose Pare 1866 GV after sword wound Berti 1895 Described GV during autopsy Berg 1904 1st successful operation Borchardt 1920 Classical triad Roselet 1930 Described radiologically Buchanan 1968 Clarify anatomical variation Tanner Etiology & methods of repair
Predisposing factors • Primary • Laxity of the supporting ligaments • Especially elongation of the gastrosplenic and/or gastrocolic ligaments • one-third of cases
Predisposing factors • Secondary Diaphragmatic defect • eventration • paraesophageal hiatal hernia • Bochdalek hernia • trauma • paralysis Congenital bands or adhesions Intestinal malrotation Pyloric stenosis with gastric distension Colon distension
Predisposing factors • Diaphragmatic defects - 43% • Gastric ligaments - 32% • Abnormal attachments, adhesions, or bands - 9% • Asplenism - 5% • Small and large bowel malformations - 4% • Pyloric stenosis - 2% • Colonic distension - 1% • Rectal atresia - 1%
Classifications • Onset - Acute Vs Chronic • Location– subdiaphragmatic / primary Vs supradiaphragmatic / secondary • Axis of rotation– organoaxial/ mesenteroaxial / combined / unclassified • Etiology– type 1(idiopathic) Vs type 2 (congenital or acquired)
Classifications • Subdiaphragmatic, or primary • not associated with diaphragmatic defects • one third of cases • Supradiaphragmatic, or secondary • associatedwith diaphragmatic defects • two thirds of cases
Classifications • Organoaxial volvulus Rotates about the cardiopyloric axis results in an upside down stomach with thegreater curve on top Obstruction may occur at the gastroesophageal junction and the pyloroantral area. 59% Mainly adult
Classifications • Mesenteroaxial volvulus Anterior rotation about an axis perpendicular to the cardiopyloric axis Greater curve remains on the bottom 29% Mainly children
Clinical Presentation • Borchardt’s classical triad (1904): • epigastric pain and distention • Non-productive vomiting • difficulty with nasogastric tube insertion
Investigations Barium study • high sensitivity and specificity • criterion standard for diagnosis • upside-down configuration of the stomach • esophagogastric junction is lower than normal. • marked gastric dilatation and the slowpassage of contrast past the site of twisting
Investigations X-Ray • findings suggestive of gastric volvulus should be confirmed with a barium study • Erect film:two air-fluid levels on the fundus - inferior, antrum - superior • Supine film: a beak where the esophagogastric junction is seen on normal images
Investigations Endoscopy • Both diagnostic and therapeutic • Mainly for therapeutic CT / MRI / USG • Not diagnostic • Consider in patient cannot tolerate endoscopy or fluoroscopy
Investigations Teague et al, BMJ 2000
Treatment • Aims: • Reduction of volvulus • Gastric fixation • Repair of predisposing factors • Open Vs Endoscopic Vs Laparoscopic Vs Combined endoscopic and laproscopic
Treatment – open surgery Open Surgery(traditional treatment >10 years ago) • Diaphragmatic hernia repair • Division of bands • Gastropexy • Partial gastrectomy (in case of necrosis) • Gastropexy with division of gastrocolic ligament (Tanner’s Operation) • Gastrojejunostomy • Fundoantral gastrogastrostomy (Opolzer’s Operation) • Repair of eventration of diaphragm
Treatment- endoscopic Endoscopic reduction Alpha-loop maneuver Tat-Kin Tsang et al ,1995 J-type maneuver D.K. Bhasin et al, 1990 • +/- gastrostomy for the fixation of stomach to the abdominal wall
Treatment – alpha loop A,B,C Survey of the stomach and gastric volvulus and formation of alpha-loop D,E,F, Completed formation of alpha-loop with the advancement of tip pf the endoscope into the antrum and uncoiling of the loop and reduction of the volvulus Tsang et al. 1995
Treatment - J-type maneuver A,B Formation of the ”J “by turn extremely up and to the right to locate the lumen C,D,E Endoscopy is maneuvered into the duodenal cap. Tip of the endoscopy is turned to right and partially locked. Endoscopy is rotated through 180o in anti-clockwise direction and withdrawn Bhasin et al. 1990
Treatment - laparoscopic • 3-ports / 4-ports / 5-ports • Reduction of Volvulus • Anchoring fundus of stomach to the diaphragm • Greater curve of the stomach to anterior abdominal wall • +/- repair of diaphragmatic defect • +/- fundoplication or/and esocardiopexy–prevent post-operative GERD • +/- gastrostomy
Treatment - laparoscopic 2 vertical lines – fundus anchored to diaphragm X – anterior gastropexy stitches A – camera, B – liver retractor, C,D,E - operating ports
Treatment - laparoscopic Phrenofundopexy Esocardiopexy Anterior gastropexy
Management - combined • Described by Arben Beqiri (1997): • Use endoscopicT-fasteners instead of PEG for anchoring • Laparoscopy - reduction of volvulus • Endoscopy - placement of T-fasteners • Less time consuming
Treatment Follow-up • Clinical • reflux symptoms • recurrent of symptoms - detection of recurrence • removal of PEG tube • Imaging – Post OT contrast study (no consensus of interval - Day 2 to 3 months)
Treatment • No RCT • rare disease (2.6/million/year) • Largest series – Teague et al in 2000 • 36 patients were recruited • Results: • Diagnostic investigation: Ba contrast (21/25) and upper endoscopy (18/21) • Conservative Tx (5), open surgery (13), laparoscopic (18) –no major complications and death • Median hospital stay: shorter in laparoscopic group than open group 6 Vs 14, p< 0.05
Clinical Scenario • Laparoscopic approach • 3-ports • Organoaxial type • No diaphragmatic hernia and eventration of diaphragm • Gastropexy • 0-Ethibon • 2 anchoring fundus to the diaphragm • 2 anchoring greater curve to the anterior abdominal wall
Clinical Scenario • Follow up: • Resume diet in D3 • Contrast study in D2 stomach in normal position no gross abnormal configuration of stomach
Conclusion • Chronic gastric volvulus is a rare disease • Require high index of suspicion in diagnosis • Pain and vomiting are the main symptoms • Barium meal is the most diagnostic tool • Can be safely treated by laparoscopic approach