Download
1 / 18
180 likes | 296 Vues
DISTAL CORONARY ARTERY DISEASE S.Venkatesan Madras Medical College. Chennai.

E N D
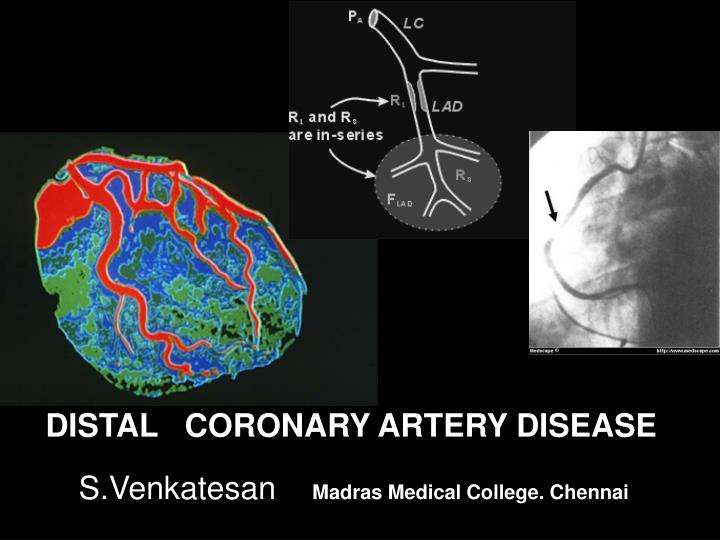
DISTAL CORONARY ARTERY DISEASE S.Venkatesan Madras Medical College. Chennai
Atherosclerosis is typically prone to occur in the proximal segments of coronary arteries. The clinical implications of proximal coronary artery disease (CAD) is well known. The real prevalence of distal CAD is largely unreported.
The aim of this study is to find out the prevalence rate of isolated distal CAD and their angiographic features.
Distal CAD definition Distal CAD was diagnosed when it occurred distal to second septal or diagonal in LAD, or in the D1 or S1 if it’s 20mm away from it’s origin. In LCX and RCA distal CAD was diagnosed when the lesions were beyond OM1 or RV branches respectively. All PDA and PLV lesions were considered distal.
All lesions more than 20% diameter stenosis were included. ( Since the aim was to detect atherosclerosis and not the obstructive CAD) Patients with one or more proximal or mid lesions were excluded
360 angiograms from our lab were reviewed sequentially . Clinical diagnosis were CSA 45%, UA35% , AMI, 20% RHD 4% . Age range was 22-73( m 56) with M : F 3.5: 1.
Risk factor profile Diabetes 15% SHT 18% Dyslipidemia 15% Smoking 12%
Isolated Distal CAD occurred in 68(19% ). It was most common in chronic stable angina .
Double vessel Distal CAD (52%). Triple vessel Distal CAD 30%. Single vessel Distal CAD (18%).
Distal CAD DVD TVD SVD
Distal cad prevalent sites The prevalent combinations were PDA -OM /D2, PDA/DI /OM ,LAD/PDA/OM Among SVD, PDA lesion was the commonest , LAD was least common.
Distal CAD Lesion characters The mean length of distal CAD was 5mm (2-14mm). The mean severity of lesion is 50%( 20-100%). Total occlusion in distal segments was a rarity 3/68. Eccentric lesions occurred in 10%. Intra coronary thrombosis and calcification was not seen in any . Luminal irregularity in distal segments was seen in about one third of patients.
SUB GROUP ANALYSIS DISTAL CAD was more prevalent in Diabetic and hyperlipidemia(26% Vs 19%)
Conclusion We conclude isolated Distal CAD occurs in significant population among CAD. (19%) It is most common in PDA followed by LCX ,OM and diagonals Least common in the LAD . The lesions generally are shorter and less severe.
Implication Our observations reveal a significant burden of atherosclerosis occurs exclusively in the distal coronary vascular bed It could have important therapeutic implication in selecting the modality of interventions.