GHRH
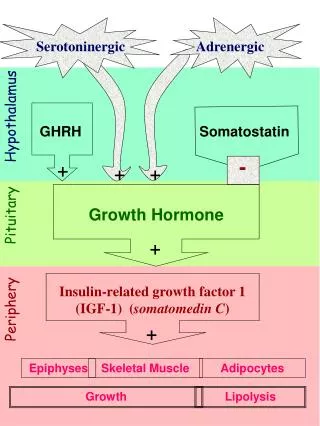
Growth Hormone. Insulin-related growth factor 1 (IGF-1) ( somatomedin C ). Serotoninergic. Adrenergic. Hypothalamus. GHRH. Somatostatin. -. +. +. +. Pituitary. +. Periphery. +. Epiphyses. Skeletal Muscle. Adipocytes. Growth. Lipolysis.

GHRH
E N D
Presentation Transcript
Growth Hormone Insulin-related growth factor 1 (IGF-1) (somatomedin C) Serotoninergic Adrenergic Hypothalamus GHRH Somatostatin - + + + Pituitary + Periphery + Epiphyses Skeletal Muscle Adipocytes Growth Lipolysis
General Mechanisms of Releasing and Inhibiting Hormones in the Hypothalamic-Pituitary Axis TRH Inhib. Dopamine GHRH G G PL-C ATP 3’5’-cAMP
Human Growth Hormone (HGH) • 191 amino acid peptide v.similar to prolactin and HCG. • Recombinant HGH 191 identical or 192 with added methionine. • Humans highly selective in responding only to HUMAN growth hormone amino acid sequence. • Other animal species don’t work. Bovine GH (as in US beef) has no known actions in humans. • Inactivated in gut if given orally: usually given sub-cutaneously. • T1/2endogenous HGHabout 25 min.
Human Growth Hormone (HGH) Indications Growth Hormone Deficiency in Children • growth less than 4 cm/yr. and • failure to respond to stimulation (e.g hypoglycaemia, arginine,clonidine, etc.) Growth Hormone Deficient Adults • controversial Treatment of Catabolic States • ICU +/- parenteral nutrition (lipolysis to mobilise fat stores) • anabolic agent (e.g. Short bowel syndrome along with parenteral nutrition). Abuse • role as doping agent in sport is controversial.
Human Growth Hormone (HGH) Adverse Effects • Creutzfeldt Jacob disease with pituitary extracts (until 1985). • Fluid retention (temporary). • Antibody formation (30% of patients) doesn’t affect efficacy. • Slipped epiphyses if growth response is very rapid. • Glucose intolerance • ?? Increased incidence leukaemia.
Somatostatin(Growth Hormone Inhibiting Hormone) • Hypothalamic inhibitor of growth hormone release. • Also found in pancreas and GIT. • Also inhibits glucagon, insulin and gastrin release. • 14 amino acid peptide. • Very short T1/2(1-3 min) in plasma. Therapeutic Analogues Octreotide(8 amino acids) • T1/280 min • 45-times more potent than somatostatin Lanreotide • T1/24.5 days • fortnightly IM injections
Somatostatin Analogues Octreotide and Lanreotide • Inhibit growth hormone secretion in acromegaly. • Cause tumour regression in acromegaly and prolactinoma. • Inhibit tumour growth in gastro-entero-pancreatic axis carcinoma (e.g. gastrinoma, glucagonoma, carcinoid tumours). • Inhibit endocrine-disorder induced diarrhoea. • Used with bleeding oesophageal varices (Octreotide) due to vasomotor effect in splanchnic circulation. • Adverse Effects: • glucose intolerance • gallstones
Prolactin Serotoninergic Hypothalamus TRH Dopamine VIP - + + + OE Pituitary + OE Mammary Epithelium Progest. Insulin Periphery Milk
Prolactin Therapeutic Uses / Preparations: • None Causes of Hyperprolactinaemia • Physiological (pregnancy & post-partum: oestrogen-stimulated) • Hypothyroidism (causing TRH excess) • Prolactinoma • Hypothalamic dopamine deficiency • Defective dopamine delivery • Lactotroph cells insensitivity to dopamine • Dopamine antagonists present Treatment of Hyperprolactinaemia • Correction of underlying cause • Dopamine analogues
Dopamine Analogues Bromocriptine • Ergot peptide alkaloid • Highly selective dopamine receptor agonist. • Weak a-adrenergic and 5-HT agonist. • Inhibits Gi-protein coupled adenylyl cyclase • Inhibits prolactin release. • Inhibits growth hormone release, especially in GH-secreting tumours which co-secrete prolactin. Dosage • once - three times daily. • Safe in first 3-weeks of pregnancy Adverse Effects • nausea (stimulation of medullary vomiting centre). • Vasospasm at high dosage • Pulmonary infiltrate in chronic use.
Dopamine Analogues Cabergoline • very long half-life of prolactin suppression allows twice-weekly dosage. • Less tendency than bromocriptine to cause nausea; probably better receptor selectivity. • Newer; less experience in early pregnancy; no reason to believe a problem exists. • Long-term adverse effects unknown
Hyperprolactinaemia from Dopamine Antagonists Remember the following commonly used drugs may cause Hyperprolactinaemia: Dopamine antagonist Anti-nausea agents: e.g. • metoclopramide (e.g. Maxolon) • prochlorperazine (Stemetil) • domperidone (Motilium) Neuroleptics / Major tranquillisers e.g. • chlorpromazine • trazodone • prochlorperazine • thioridazine.