Download

1 / 76
820 likes | 1.29k Vues
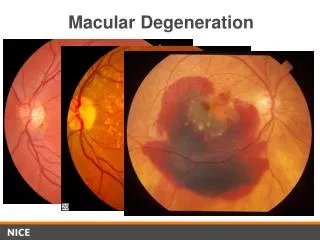
بسم الله الرحمن الرحيم. Macular Invovement in Posterior Uveitis. F. Kianersi M.D 1386 / 8 / 3. Posterior Uveitis is one of the vision threatening diseases especially when the Macula is involved. Several Posterior Uveitic entities involve the Macula, which can either be:

E N D
بسم الله الرحمن الرحيم Macular Invovement in Posterior Uveitis F. Kianersi M.D 1386 / 8 / 3
Posterior Uveitis is one of the vision threatening diseases especially when the Macula is involved. • Several Posterior Uveitic entities involve the Macula, which can either be: • Infectious or • Non-Infectious.
Infective causes Toxoplasmosis b. Toxocariasis c. Tuberculosis d. Herpetic Common Posterior UveiticEntities Invoving Macula
Acute Posterior Multi Focal Placoid Pigment Epitheliopathy (AMPPE) Multiple Evanescent White Dot Syndrome (MEWDS) Macular Geographic Helicoid Peripapillary Choroidopathy Birdshot Choroidopathy Presumed Ocular Histoplasmosis Syndrome (POHS) Retina Pigment Epithelitis (Krill's disease) Punctate Inner Choroidopathy Sub Retinal Fibrosis and Uveitis Syndrome Harada's disease Sympathetic Ophthalmia Multifocal Choroiditis Sarcoidosis Behcet Disease. Common Posterior UveiticEntities Invoving Macula Non-Infective Causes
TOXOPLASMOSIS • It is the most common cause of Posterior Uveitis in the Immunocompetent patients. • Toxoplasmosis is caused by the obligate Intra-Cellular Protozoan Toxoplasma Gondii.
Most often is Congenital. • Toxoplasmic Retinochoroiditis is Unilateral in 72 to 83% of the cases. • Ocular Toxoplasmosis occurs from activation of cysts deposited in or near the Retina.
Congenital Toxoplasmosis • Most commonly acquired during the 3th Trimester of Pregnancy. • Infants are usually asymptomatic.
Peripheral Retinochoroidal scars are the most common ocular finding occurring in 82% of the patients. • However, Toxoplasma has a strong predilection for the Posterior Pole, particularly the Macular region.
Typical Congenital Toxoplasmic Retinochoroiditis Macular Cicatricial Lesion, consisting in: Radial Deposition of Pigment around a Central Necrotic Zone.
Recurrent lesions frequently develop at the borders of the old Toxoplasma scars, so called Satellite lesions.
A Yellowish White or Grey Exudative lesion is seen with ill defined borders because of surrounding area of Retinal Edema. • Adjacent Choroiditis, Retinal Vasculitis, Hemorrhage and Vitritis may be seen.
An Active lesion accompanied by a severe Vitreous Inflammatory reaction will have the classic “Headlight in the Fog" appearance.
Healed Scar typically has well defined borders with Central Retinochoroidal Atrophy and peripheral RPE hyperplasia.
Toxoplasmosis Neuroretinitis Active lesions localized to the Juxtapapillary region, aggressively involving the Retina and Optic Nerve.
Toxoplasmosis Neuroretinitis Papillitis with Disk Hemorrhages, Venous Engorgement and overlying Vitritis.
Toxoplasmosis Neuroretinitis Later, a Juxtapapillary Retinochoroiditis and Macular Star develop.
Toxoplasmosis Neuroretinitis Toxoplasma Neuroretinitis is an Ophthalmic Emergency and requires prompt treatment.
Complications of Ocular Toxoplasmosis • Secondary Glaucoma, • Cataract, • Vitreous Hemorrhage, • Retinal Detachment, • Choroidal Neovascular Membrane (CNV), • Cystoid Macular Edema (CME), • Ocular Vascular Occlusions, • Optic Atrophy.
Diagnosis • Diagnosis of ocular Toxoplasma is based mainly on clinical findings. • Serological studies are helpful in suspected cases or the ones with atypical presentation.
Treatment • Despite recent advances, an ideal combination that destroys the Tissue Cysts and prevents recurrence has not been found. • Current therapies are targeted mainly at the Active disease.
A combination of the following drugs are used: • Pyrimethamine: Loading dose: 100 mg (1st day), followed by 25 mg once daily. • Sulfadiazine: 4 Gr daily divided in every 6 hours. • For 4 to 6 weeks. • These two drugs work synergistically against the Tachyzoite form of T gondii.
Other drugs used in various combinations include: • Clindamycin: 150-450 mg/dose every 6-8 hours, maximum dose: 1.8 gm/day. • Trimethoprim + Sulphamethoxazol (Co-Trimoxazole): 160 mg/800 mg (one tablet) twice daily. • Spiramycin: 2 gr/day in two divided doses. • Azithromycin: Loading dose 1 G (1st day), followed by 500 mg once daily for 3 weeks.
Oral Corticosteroids Oral corticosteroids must be initiated at least 24 hours after starting anti parasitic drugs.
Therapy regimens used during Pregnancy: • Spiramycin: 2 gr/day in two divided doses. • Treatment of the Mother reduces the likelihood of Congenital transmission.
Standard regimen for newborns Pyrimethamine + Sulfadiazine + Folinic acid
Management • Folinic acid for decreasing the likelihood of Leukopenia and Trombocytopenia. • Weekly exam of CBC and PLT.
Surgical Treatment • Pars Plana Vitrectomy: to remove Vitreous Opacities, or to relieve the persistent Vitreo-Retinal traction. • Scleral Buckling: in cases complicated with Retinal Detachment.
Prognosis In cases where Optic Nerve or Macula is spared from the active disease Prognosis remains Good.
Poor Prognosis Profound Visual Loss: Macular Scars, Secondary Glaucoma, Retinal Detachment,
Poor Prognosis Profound Visual Loss: Macular Scars, Secondary Glaucoma, Retinal Detachment, CNV.
Toxocariasis is an infection caused by the accidental ingestion of: Larvae of the Dog Round-Worm, Toxocara Canis.
Clinical Features • Granuloma in the Peripheral Retina and Vitreous.
Clinical Features • Granuloma in the Peripheral Retina and Vitreous. • Posterior Pole Granuloma.
Clinical Features • Granuloma in the Peripheral Retina and Vitreous. • Posterior Pole Granuloma. • Chronic Endophthalmitis.
Posterior Pole Toxocariasis Whitish or Grayish-White in Colour
size of Posterior Pole Toxocariasis Less than One Disk Diameter Involvement of the Entire Macular Region
Location of Posterior Pole Toxocariasis Juxtapapillary Subfoveal Location
Diagnosis The diagnosis of Ocular Toxocariasis is based on Clinical findings and the serological correlations.
Treatment • Medical treatment is directed toward the inflammatory response that produces Structural Damage and decreased vision. • This includes initial treatment with Topical or Systemic Steroids. • Antihelminthic therapy for Ocular Toxocariasis do not alternatural course of the disease.
Acute Posterior Multifocal Placoid Pigment Epitheliopathy(APMPPE - AMPPE)
Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE - AMPPE) • Sudden, Painless Loss of Vision, usually Bilateral. • A flu-like prodrome consisting of Fever, Malaise and Headache precedes most cases of AMPEE.
Fundus Examination Multiple Round, Circumscribed, Flat, Yellow White Sub-Retinal lesions involving the RPE.