Download
1 / 40
440 likes | 951 Vues
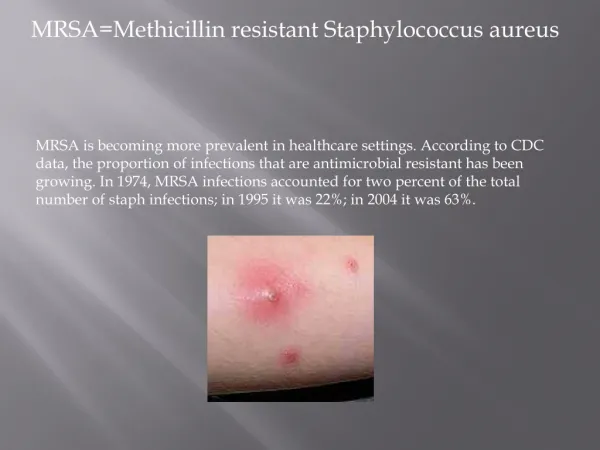
Methicillin Resistant Staphylococcus Aureus. Barbara Jennings-Spring Seminar in Molecular Biology 360 Smith College. What Is MRSA?. MRSA Is “Methicillin Resistant Staph Aureus”

E N D
Methicillin Resistant Staphylococcus Aureus Barbara Jennings-Spring Seminar in Molecular Biology 360 Smith College
What Is MRSA? MRSA Is “Methicillin Resistant Staph Aureus” *It is a bacteria that is resistant to a synthetic penicillin methicillin. Staph aureus colonizes skin, nasal passages, and many other mucous membranes. *Also causes a variety of disseminated, lethal infections in humans. * It has the ability to transfer resistant genes easily to other species directly and indirectly *Overuse of antibiotics is the one of the major reasons for the evolution of MRSA
Overview To gain a better understanding of the molecular mechanisms involved with (MRSA) and how biotechnology continues to combat this super-bug in hospitals and communities throughout the world.
Research History Of MRSA • The Basic Biology Of Staphylococcus Aureus • Molecular Basis For Virulence • Clinical Presentation Of Disease • Detection Of Pathogen • Biotechnology Treatments • Public Health Control Strategies • Political And Social Impediments • bullet point
History Of Antibiotic Resistance • 1941 Penicillin • 1943 Streptomycin • 1945 Cephalosporins • 1950 Tetracycline • 1952 Erythromycin • 1956 Vancomycin • 1960 Methicillin • 1962 Lincomycin • 1962 Quinolones • 1970 Penems • 1980 Monobactams • 2010 Is this the end of an antibiotic era???
The Basic Phenotypic Characteristics Of Methicillin Resistant Staphylococcus Aureus • Gram positive • Non-motile • Spherical • Grows in chains • Resembles clumps of grapes • Golden color • Hemolytic pattern on blood agar • Produces coagulase and catalase enzymes
The molecular genetics of antimicrobial resistance includes three main pathways: • Microevolutionary changes-a single point mutation • Macroevolutionary change- rearrangements occur • Acquisition of foreign DNA
What are some examples of how single point mutations occur over time? • Beta lactamases will confer resistance to B- lactams (penicillins, cephalosporins) • If you get a single point mutation (substitution of base pair) that involves the target action of PCN or the cephalosporin drug, you will extend the spectum of action of that B-lactamase enzyme • so that a broad range of the cephalosporin or penicillin family will show resistance instead of one single cephalosporin or penicillin family • Mutations on the rpoB gene (RNA polymerase) alters antibiotic binding site, preventing drug action.
What Are Some Examples Of Macro Evolutionary Changes With Resistance? • Rearrangement of DNA segments-by transposons • Transposon—”Jumping Gene” that contributes to antibiotic resistance • Transposons- Contain genes that are for the coding of antibiotic resistance
How is the Acquisition of Foreign DNA from other species accomplished? • Conjugative plasmids: Found inside cytoplasm. • Possess the ability to transfer resistance genes to the same and different species Horizontal gene transfer is common in bacteria and is accomplished by the process known as Transformation in Staph. aureus.
Examples of horizontal Gene Transfers (HGT) • http://www.bioteach.ubc.ca/Biodiversity/AttackOfTheSuperbugs/
How Staph Aureus acquires resistance to methicillin • http://www.jci.org/cgi/content/full/114/12/1693/F1 http://www.jci.org/cgi/content/full/114/12/1693/F1
Mechanism of Antibiotic Resistance in MRSA • http://www.bioteach.ubc.ca/Biodiversity/AttackOfTheSuperbugs/
Important Virulence Factors for MRSA: Cell Wall Structures • Cytoplasmic membrane- osmotic barrier • Consists of thick polysaccharide capsule (slime layer; adhesin). Capsules are just tricks to avoid host defenses • Petidoglycan-Used for osmotic stability so bacterial cell wall does not burst due to hypertonic states. • Protein A- immunological disguise. Inhibits oponization , Binds IG’s, leukocyte, chemoattractant, anticomplementary. • Techoic Acid-Acts as a receptor for bacteriophages. Attachment site for mucosal cell receptors.
Invasive enzymes As Other Virulence Factors • Coagulase Complex-Produces enzymes that coagulate blood and seal off infection • Protease,lipase, & DNase provide nourishment for MRSA bacterium • FAME-Important in abscess formation. Also it could change anti-bacterial lipids and prolong survival of MRSA in wound. • Staphylokinase-Plasminogen activator enzyme that lyses fibrin clots • Hyaluronidase-It is the spreading factor; hydrolyzes haluronic acid in synovial joints
Virulence Factors Cont: Extracellular Products and Toxins (hemolysins) Of MRSA Invasion • Leukocidins-The name implies their job! Leukocidins kill wbc’s. Membrane damaging toxin • Alpha, beta, delta toxin-binds to cell surface, forms pores leaks. • Superantigens: (type 1 toxin) Toxic shock syndrome toxin (TSST-1) • Staphylococcal Enterotoxin-food poisoning • Exfoliation toxin-scalded skin syndrome
Virulence Factors Cont: Mechanism Of Superantigens And The Stimulation Of Cytokine Release http://textbookofbacteriology.net/staph.html
Summary of Virulence Determinants Of Staph. Aureus • http://textbookofbacteriology.net/staph.html http://textbookofbacteriology.net/staph.html
Source of MRSA Infections • Some infections are caused by own epithelial flora-self contamination • Nasal carriage most common • Hospitals • *Dirty hands, towels, and daycare • Airborne?????
Predisposing Factors Of Host Resistance • Integument injury via surgery • Burns and trauma • Foreign objects like indwelling catheters, metals, sutures, implants • A history of chronic bacterial infections with multiple rounds of antibiotics • Hormonal changes and stress • Immunocompromised (AIDS, Diabetes, Chemo)
Clinical Manifestations Of MRSA • The lesion usually starts out as an small cut or break in the skin. The lesions can range from small abrasions to large, gaping abscesses • Even the most benign localized abrasion (from tampon insertion) can become the fuel for a devastating, disseminated MRSA systemic infection that do not respond to multi-antibiotic combinations
MRSA Infections Go Everywhere • Integumental and soft tissue • Suppurative arthritis-first causative agent • Osteomyelitis-First causative agent • Bacteremia-First causative agent • Pneumonia • Acute and chronic Endocarditis-#1 • Bacterial Meningitis-first causative agent
Menstrual Toxic Shock By MRSA • Most major organs fail with disseminated MRSA (TSS-1) www.web.net/terrafemme/ cashnightmare.htm
More MRSA Infections • Toxic shock Syndrome-Super absorbent tampons- #1 causative reason • Urinary tract Infections • Scalded skin syndrome and impetigo from picking pimples • Food poisoning-Enterotoxin A in spoiled or contaminated food.
Carbuncle(Boil) • tahilla.typepad.com/.../ super_bug_091404.jpg
44 y/o IV drug abuser with back pain and Staph Osteomyelitis of lumbar spine • . Staph osteomyelitis and discitis involving L5, with extension across the L4-5 disc to erode L4 and extension into S1. The L5 vertebral body is destroyed. (33.210, 33.250, diskitis) Case 72
Classic Toxic Shock: Scalded Skin Syndrome www.aafp.org/afp/ 20000815/804.html
Staph. Aureus Impetiigo • Don’t pick your face!!!!! www.med.sc.edu:85/ fox/staph-impetigo.jpg
Getting A Lab Diagnosis For MRSA • http://jcm.asm.org/cgi/content/full/38/6/2378 MRSA
How Accurate Can Your Diagnosis Of MRSA Be? http://jcm.asm.org/cgi/content/full/38/6/2378
Current Drug Treatments For MRSA • [Methicillin-resistant] –MRSA Drugs of Choice: • Linezolid(protein synthesis inhibitor), Daptomycin, • Vancomycin • Alternatives: Synercid, Rifampin • Third-Line agents: TMP-SMX
Drugs In Development • Oritavancin-can be given once daily • Tigecyclin-orally broad antimicrobial activity • Dalbavancin- Currently undergoing clinical trials. Has long half-life so it can be given once per week (FDA, 2005)
How Close Is Staph Vaccine? • Pretty close. The results of the phase 3 testing of the vaccine (Staph VAX) will be presented soon according to the NIH.
Public Health Response-What Is Being Done To Combat MRSA? • The CDC provides technical help and referrals to state and local health departments, doctors, nurses, and other professionals • The CDC provides national program of surveillance for serious infections with MRSA. • CDC launched evidence-based educational campaign to prevent antimicrobial resistance • CDC building national resource library to identify genetic patterns or relationships • CDC researching the role of staph toxins-to provide answers for hospitals and researchers • *For more info go to www.cdc.goc
What can you do to prevent MRSA from attacking You? • Keep draining infections of skin, covered with clean dry bandages • Talk to your physician about wound management techniques • Advise family to wash hands frequently with soap and water, count to at least “20”,especially after dressing a gaping wound. • Avoid sharing personal items such as towel, razors, bed linens with people who have sores or have come home from the hospital recently • Wipe objects down with alcohol. • If you are in the hospital please advise you nurse or physician to wash their hands before touching you or your hospital equipment
Rising Rates Of Resistant Bacterial Infections=Rising Budget
That’s All Folks!! Any Questions???? • Staph cells attaching photo courtesy of Dr. Sharon peacock- University of Oxford
References • 1 Mitchell, David.MRSA.”what’s New”. Inoculum. Volume 8, number 2 (1999) 1-12. • 2 textbookofbacteriology.net/resantimicrobial.html • 3 healthsciences.columbia.edu/ dept/ps/2007/mid/2006/transcript_02_mid22.pdf • 4 http://www.bioteach.ubc.ca/Biodiversity/AttackOfTheSuperbugs • 5. Foster, Timothy. The staphylococcus aureus “superbug”.J. clin Ivestigation • Volume number114 (2004) 1693-1696. • 6. www.channing.harvard.edu/4a.htm • 7. ww.ncbi.nlm.nih.gov. • 8. www.aafp.org/afp/ 20000815/804.html • 9. Journal of Clinical Microbiology, June 2000, p. 2378-2380, Vol. 38, No. 60095-1137/04.00+0 • 10. www.FDA.com (FDA archives) • 11.www.postgradmed.com/issues/2001/10_01/hoel.htm12. www.cdc.gov/ncidod/hip/aresist/mrsa_CDCactions.htm • 13. www.medscape.com