Download
1 / 29
300 likes | 439 Vues
The role of randomized trials in testing interventions for the prevention of youth suicide. C. Hendricks Brown, Peter A. Wyman, Joseph M. Brinales, & Robert D. Gibbons. International Review of Psychiatry, Dec 2007;19(6):1-15. Introduction. Suicide recognized as a major public health problem

E N D
The role of randomized trials in testing interventions for the prevention of youth suicide C. Hendricks Brown, Peter A. Wyman, Joseph M. Brinales, & Robert D. Gibbons International Review of Psychiatry, Dec 2007;19(6):1-15
Introduction • Suicide recognized as a major public health problem • The third leading cause of death among American youths. • 9% of American high school students reporting a suicide attempt • 2.6% of youth attempts are serious enough for medical attention. • Burden of suicide behavior • Death from suicide • Suicide attempts are 10-40 times as prevalent as completed suicides. • Deep impact on surviving family and friends, the loss to society due to a young person’s death.
Introduction • The prevention of suicide to be a priority for many countries. • The US Healthy People 2010 goals • The reduction of deaths from suicide by 2010 from 10.5-10.8/100 000/year (1998 to 2003) to 4.8/100 000.
Epidemiological findings on risk and protective factors for suicide: Targets for youth suicide prevention programmes • Good epidemiologic studies that have tracked suicide rates over time, and identified • Which population are at elevated risk • Which risk and protective factors could be targeted for preventing suicide
Targeting populations with elevated risk • Less common in ethnic groups that have strong religious prohibitions against suicide. • Attempts are higher in females, males have much higher suicide mortality in most regions except in rural China. • Ideation and attempts tend to occur more often in those youths whose parents also experienced suicidality • Suicide attempts are far more common among males whose sexual orientation is bisexual/homosexual. • Suicide is more common in rural compared to urban.
Prevention strategies addressing availability of factors linked to suicide • Official rates of youth suicide in the USA have nearly tripled since the 1950s through 1998 • Increases in alcohol and substance abuse • Increased availability of firearms • The programmes can potentially lead to a reduction in youth suicide • Reduce sales of alcohol to youths • Reduce access to lethal means
Changing prevalence of youth suicide • The youth suicide rates especially for males have been decreasing recently in the USA since the mid 1990s • May be due to the large reduction in drug use • But youth suicide had increased 14% in 2004 • The large drop in pediatric prescriptions following the FDA public health advisory in 2003 and black box warning in 2004
Treatment for depression and other mental disorders: Implications for prevention of suicide • Increase treatment for depression • The primary strategy identified in Healthy People 2010 • 1/4 of US adults who are depressed receive treatment in 1997 • Treatments of depression • Antidepressant medication and psychotherapy • Psychosocial as well as non-clinical prevention approaches are essential. • Prescriptions are declining in youths • Lack of acceptability and accessibility to mental health services in many area.
The role of randomized field trials to evaluate programmes in community-based programmes for preventing youth suicide • Randomized field trials (RFTs), used to test interventions in realistic community settings. • RFTs often use group-based randomization, for example at the level of classrooms or schools. • Suicide intervention require large sample sizes and/or long follow-up periods to determine whether deaths are significantly reduced by exposure.
The role of randomized field trials to evaluate programmes in community-based programmes for preventing youth suicide
The role of randomized field trials to evaluate programmes in community-based programmes for preventing youth suicide • Alternatives to lowering the required size or length of the study • To select populations that have higher rates of suicide. • Adolescents in rural US counties (20/100 000) • To replace self-inflicted mortality with a surrogate endpoint of self-reported attempted suicide, medical records of an attempt, or suicidal ideation.
Three promising psychosocial prevention strategies amenable to evaluation through randomized trials • Tertiary prevention of suicide in clinic or institutionally identified high-risk youths. • Selective or secondary prevention of suicide in difficult to identify of non-clinic high-risk communities. • Protective, universal strategies for the entire population of youths.
Tertiary prevention of suicide in clinic or institutionally identified high-risk youths • Psychosocial prevention would be to lessen suicide risk. • A number of interventions have been tested. • Most low intensity or short programmes, such as CBT only in an inpatient setting are generally ineffective. • Longer, more intense interventions can be effective in reducing suicidal behavious. • The low frequency of these condition in the population demonstrates intervention with these high-risk youths alone will not lead to a large reduction in youth suicide.
Tertiary prevention of suicide in clinic or institutionally identified high-risk youths • Provide a specific preventive intervention to youths at elevated risk for suicide. • A randomized trial underway now. • Suicidal youths and families who use crisis hot-lines are providing a means of self identification. • One study on crisis hotlines is now underway
Secondary prevention of difficult to identify, high-risk youths • The vast majority of suicidal youths do not come to the attention of the mental health system or their schools. • Uses multi-stage psychiatric screening to identify those youths who are at high risk within the general population. • Gould and colleagues found asking about suicide dose not cause increased distress. • Gatekeeper training to identify high-risk youths • Learning warning signs about suicide • Asking the person if they are thinking of killing themselves
Protective strategies for an entire youth population • A school-based randomized trial that just beginning will test the Sources of Strength programme. • Implemented in half of the schools after they receive gatekeeper training, Sources of Strength aims at changing peer norms about youths seeking help. • Successful norm change can help youths recognize that suicidality is not a normal condition that must be endured, nor is suicide a common solution to problems they feel.
Protective strategies for an entire youth population • Two other classes of pupulation-based programmes • A randomized trial was conducted to evaluate a programme that helps youths identify signs of depression, and found reduced self-reported suicidal attempts. • The second approach uses prevention to target known risk factors for suicide, such as drug abuse, aggressive behaviour, etc. • One randomized trial has been shown to reduce aggressive behaviour, delinquency and drug abuse, and reduce suicidal ideation and attempts by 50%.
Two new approaches to conducting population-based randomized field trials to prevent suicide • Dynamic wait-listed design • Multi-trial follow-up design
Dynamic wait-listed randomized design • A randomized trial is now underway to test the QPR gatekeeper training programme in 32 middle and high schools, 2500 staff, and 50 000 students in Georgia. • The school district where this trial began had already decided to train all school staff. • The primary outcome of this trial was referral to school for suicidality. • This design called for random assignment of 16 of the schools to the early training condition and the remaining 16 schools to later training.
Multi-trial follow-up design • The study differs in two important ways from a typical meta-analysis • New data regarding the nature of death of prevention trial decedents are collected on each trial from a National Death Index search. • The analyses require the use of individual level de-identified data, which is not needed for standard meta-analyses.
Multi-trial follow-up design • There are now more than 60 well-designed preventive field trials that have tested preventive intervention. • Together they have involves more than 37 000 children. • None of these specifically target suicide. • Many of the studies have long follow-up periods. • Represent an untapped potential for understanding how malleability of early risk factors can affect suicide
Discussion • Progress in understanding what works in suicide prevention has been regrettably very slow. • Randomized trials are a great asset in evaluating prevention programmes. • None of preventive trials has a chance of reducing the population level of suicide below 5%, because the proportion who have these risk factors is very small. • Population-based prevention programmes provide the best opportunities for making dramatic reductions in suicide.
Discussion • Two main challenges in conducting randomized trials in suicide prevention research • Require statistical solution • Using a multi-trial follow-up design of the more than 100 000 youths. • A partnership between community leaders and researchers is essential. • Dynamic wait-listed design, better served the training demands in the school district as well. • One important place where large randomized trials may be able to take place is in rural and tribal areas in the USA.
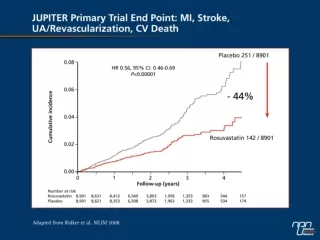
Questions • The FDA, in its review and meta-analysis of 24 placebo-controlled trials, concluded antidepressant medication pose 2-fold (4% vs 2%) • Youth suicide has increased 14%
Questions • Psychosocial as well as non-clinical prevention approaches are essential. • Prevention approaches conducted in China
Strategies reducing suicide rate in China • Tertiary • Psychiatric treatment programme • Provide for psychiatric service • Secondary • Identify high-risk youth • Gatekeeper training • Primary • Reduce sales of alcohol to youths • Reduce access to lethal means, such as pesticide
Gatekeeper training programme • Challenge in China • No place to refer • Prevention hardly accepted by individuals themselves or their relatives • Refused to accepted free cognition-behavior therapy in Huairou, Beijing • Confidentiality • Who will keep the psychological files • Independent counseling is suggested • How to identify individuals at high risk of suicide