Download
1 / 21
210 likes | 371 Vues
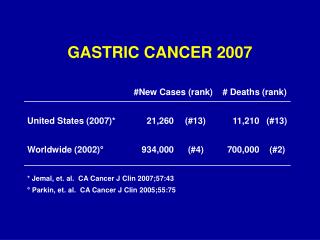
Redefining the treatment of gastric cancer with Xeloda. Sheela Rao The Royal Marsden Hospital, London and Surrey, UK. Korean 1. (n=44). 1 250mg/m 2 twice daily d1–14 q3w. Mexican 2. (n=18). Japanese 3. (n=55). 825mg/m 2 twice daily d1–21 q4w. Japanese 4. (n=32).

E N D
Redefining the treatment of gastric cancer with Xeloda Sheela Rao The Royal Marsden Hospital,London and Surrey, UK
Korean1 (n=44) 1250mg/m2 twice dailyd1–14 q3w Mexican2 (n=18) Japanese3 (n=55) 825mg/m2 twice daily d1–21 q4w Japanese4 (n=32) Xeloda monotherapy: effective and well tolerated in advanced gastric cancer (AGC) Response rate (%) Grade 3/4 AEs (≥5%) Xeloda regimen 34 HFS (9%) 25 HFS (5%) 26 HFS (13%) 19 Hyperbilirubinaemia (6%) 1. Hong YS et al. Ann Oncol 2004;15:134472. Leon-Rodriguez E et al. Ann Oncol 2002;13(Suppl. 5):191 (Abst 708)3. Sakamoto J et al. Anticancer Drugs 2006;17:2316 4. Koizumi W et al. Oncology 2003;64:2326
Phase III study: XP vs FPXeloda + cisplatin vs 5-FU + cisplatin RANDO MIS ATION XP Xeloda1000mg/m2 bid d114 q3w Cisplatin 80mg/m2 3-hour i.v. infusion n=156 Advanced and/ormetastatic gastric cancer n=316 FP 5-FU c.i. 800mg/m2 d15 q3w Cisplatin 80mg/m2 3-hour i.v. infusion n=160 • Primary end-point: non-inferiority in PFS Kang Y et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4018)
XP vs FP: non-inferior PFS Estimated probability 1.0 Median PFSmonths (95% CI) 5.6 (4.9–7.3) 5.0 (4.2–6.3) 0.8 XP (n=139) FP (n=137) 0.6 HR=0.81 (95% CI: 0.63–1.04) Compared to HR upper limit 1.25,p=0.0008 0.4 0.2 0.0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 Months Per-protocol analysis Kang Y et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4018)
XP vs FP: trend to superior PFS Estimated probability 1.0 Median PFSmonths (95% CI) 5.6 (4.8–6.9) 5.0 (3.9–5.7) 0.8 XP (n=160) FP (n=156) 0.6 HR=0.80 (95% CI: 0.63–1.03)Test for superiorityp=0.0801 0.4 0.2 0.0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 Months Intent-to-treat analysis Kang Y et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4018)
Superior response rate with XP vs FP Kang Y et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4018)
XP (n=156) FP (n=155) Comparable AEs with XP vs FP Common (≥3%) grade 3/4 AEs Patients (%) 40 30 20 10 0 HFS Nausea Anaemia Vomiting Diarrhoea Stomatitis Leucopenia Neutropenia Kang Y et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4018)
XP efficacy similar in German study 1. Moehler M et al. Proc Am Soc Clin Oncol 2006 (Abst 4032) 2. Kang Y et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4018)
REAL-2: Xeloda vs 5-FU and oxaliplatin vs cisplatin • Primary end-point: overall survival • 2x2 design with ECF as standard arm RANDO MIS ATION Epirubicin Cisplatin Xeloda n=250 Epirubicin OxaliplatinXeloda Advanced oesophagogastriccancer n=1002 n=244 Epirubicin Cisplatin Fluorouracil n=263 Epirubicin Oxaliplatin Fluorouracil n=245 1. Sumpter K et al. Br J Cancer 2005;92:197683 2. Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
REAL-2: primary end-point met non-inferior overall survival, Xeloda vs 5-FU Estimated probability 1.0 0.8 0.6 HR=0.86 (95% CI: 0.80–0.99)Compared with HR upper limit 1.23, p<0.0001 0.4 0.2 0.0 0 12 24 36 60 72 48 Months Per-protocol analysis Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
REAL-2:superior overall survival with EOX vs ECF Estimated probability Overall survival(months) 11.2 9.9 1.0 EOX ECF 0.8 0.6 HR=0.80 (95% CI: 0.66–0.97), p=0.020 0.4 0.2 0.0 0 6 12 18 30 36 24 Months Intent-to-treat analysis Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
REAL-2: good safety profiles with Xeloda-based regimens Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
REAL-2: good safety profiles with Xeloda-based regimens Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
REAL-2: good safety profiles with Xeloda-based regimens Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
REAL-2: good safety profiles with Xeloda-based regimens Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
REAL-2: good safety profiles with Xeloda-based regimens Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
REAL-2: good safety profiles with Xeloda-based regimens Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
Docetaxel/Xeloda/cisplatin (DXP): active in first-line AGC Phase III Phase II 1. Moiseyenko V et al. Proc Am Soc Clin Oncol 2005 (Abst 4002)2. Kang Y-K et al. Proc Am Soc Clin Oncol2004 (Abst 4066)
Grade 3/4 AEs: potentially less haematological toxicity with Xeloda Patients (%) 100 TCF (n=221) Phase III 80 DXP (n=40) Phase II 60 40 20 0 HFS Febrileneutropenia Platelets Anaemia Lethargy Vomiting Neuropathy Neutropenia 1. Moiseyenko V et al. Proc Am Soc Clin Oncol 2005 (Abst 4002)2. Kang Y-K et al. Proc Am Soc Clin Oncol2004 (Abst 4066)
Progress so far: overall survivalwith first-line AGC regimens 1997 BSC1 FAMTX1,2 FP1,3,4,6 ECF2,6/EOF7 MCF5/IF3/TCF4 XP6/ECX/EOX7 2006 4 6 8 10 12 Months 1. Vanhoefer U et al. J Clin Oncol 2000;18:2648–57; 2. Waters JS et al. Br J Cancer 1999;80:269–72; 3. Dank M et al. Proc Am Soc Clin Oncol. 2005 (Abst 4003); 4. Moiseyenko V et al. Proc Am Soc Clin Oncol 2005 (Abst 4002) 5. Ross P et al. J Clin Oncol 2002;20:1996–2004; 6. Data on file F Hoffmann La-Roche 7. Cunningham D et al. Proc Am Soc Clin Oncol 2006 (Abst LBA4017)
Xeloda: a highly effective, safe and convenient oral therapy for gastric cancer • Effective and simple with: • cisplatin • oxaliplatin • docetaxel • paclitaxel • triple combinations • Similar safety and efficacy profile to infusional 5-FU • Extensive phase III programme is evaluating Xeloda in: • adjuvant therapy • advanced/metastatic disease