Download
1 / 26
260 likes | 268 Vues
Improve patient safety and management of insulin therapy with a standardised insulin prescribing chart. Includes guidelines for insulin administration, management of hypo and hyperglycaemia, and safer use of supplemental insulin.

E N D
Adult Standardised Subcutaneous Insulin Prescribing Chart August 2013
Case for Change • Insulin is a high risk medication • Reported in top 10 high alert medicines worldwide • Nearly 3000 incidents in IIMS • Variation in insulin charts, charting; prescription, administration and documentation • Variation in access to specialist services and glycaemic management guidance • Mobile workforce • Need to improve management and patient safety • Risk minimisation for patients
Methodology • Review of NSW and national charts • Widespread clinical input • Developed standardised chart • Pilot - Ryde and Royal Prince Alfred • State wide consultation - parallel to State Forms process • Chart revised • Endorsed by Medication Safety Expert Advisory Committee (MSEAC)
What does it mean for me? • Separate chart from NIMC • Use in adult acute inpatient settings • Intravenous and specialty charts - unchanged • Document and use differently • All glycaemic information linked: • Prescription and administration • Easier referral to readings • Access to best practice guidelines; at bedside • Standardised chart = standardised practice; communication, documentation and interpretation • Better patient care
Key principles • Combined monitoring and guidelines - minimise delay in management decisions • Clinicians without local guidelines have clear guidelines for: • Insulin prescription • Insulin administration • Management of hypo and hyperglycaemia • Safe use of supplemental insulin • Do not take the place of local guidelines or policies • Reduced risk of error
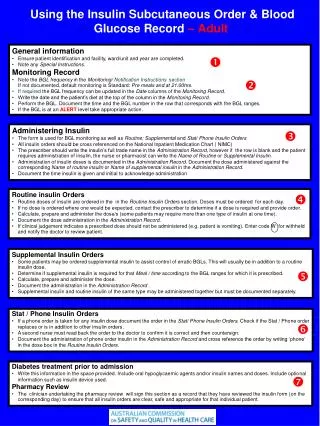
Four Sections • Page 1, including top of page 3: • Patient Identification and demographics • Alerts • Codes for not administering • Instructions • Guidelines for prescription and administration • Special instructions • Page 2 and 3: • Regular, supplemental, once only and telephone orders • BGL and ketone monitoring • Page 4: • Guidelines for glycaemia management
Patient Identification and demographics • All charts require ID label affixed consistent with NIMC • MRN • Name (family and given) • Gender • DOB • Medical Officer (MO) • Address • Location
Allergies and Adverse Drug Reactions (ADR) • Clinical staff to complete Allergies and ADR • Select Nil Known, Unknown or; • If allergy exists document: • Name of drug/substance • Reaction details • Person documenting required to: • Sign • Print name and; • Date the entry
Alerts • Prescriber document who to notify if certain criteria met e.g. BGL or ketones out of range • If no alerts select Nil • All entries signed and dated • If alert changed- cross out, sign and date it and enter new alert • Enter details in health care record
Reason for not administering • Complete when unable to administer insulin • Codes to be circled • If dose refused, notify prescriber • If withheld, document reason in health care record • If not available - obtain supply or contact prescriber
Instructions • The chart is used for: • All insulin prescriptions, except IV • Recording BGL and ketones, for patients on subcutaneous insulin • Specify frequency of monitoring (page 3) • Unstable BGLs require more frequent monitoring • All patient management must also be documented in health care record
Guide: Prescription & Administration • Daily review and prescription recommended: • May order ahead if glycaemic status stable • Modify requirements - Peri-operative and modified diets • Target BGL range 5-10mmol/L, except pregnancy • Do not re - write units, it is pre printed • Orders: • No alterations to original order • Discontinue by line through insulin name, 2 oblique lines in administration column on day of discontinuation, sign and date • Abdomen is preferred injection site
Additional information and instructions • Indicate if patient is on: • Insulin pump • Other diabetes medication • Special instructions: • To communicate information at bedside e.g. supervise using insulin pen • Can be completed by any staff member NB: All patient management must also be documented in the patients health care records
Daily orders- may be in advance if stable • Regular subcutaneous orders must contain: • Type of insulin • Date prescribed • Frequency • Time of administration • Dose • Prescriber’s signature and name printed • Prescribers contact • Administration record must contain: • Time given • Initials of administrator • Initials of 2nd person checking • Before administering regular insulin check if supplemental insulin is ordered and needed • NB: Two staff to initial and record time given, one of which must be a registered nurse
Supplemental Insulin • Guidelines page 4 • Daily review and adjustment of regular insulin during acute phase of illness • Not a replacement for regular insulin doses • Best given before a meal, in addition to usual insulin • If repeated doses needed - consider adjustment of regular doses • Prescribed based on preferred range in space provided
Supplemental Insulin prescription • Order must contain: • Type of insulin • Date prescribed • Time of administration- before meals or specify • Dose for each BGL threshold • Prescribers signature, name and contact
Supplemental Insulin administration • Administration record must contain: • Date • Time • Dose • Initials of administrator • Initials of 2nd person checking NB: One nurse must be a registered nurse
Page 3 • Blood glucose and ketone monitoring • Frequency selected • Hypo record and treatment comments (right hand side) • Once only subcutaneous insulin (bottom) • Telephone orders • 4 Most be signed within 24 hrs
Patients on subcutaneous insulin only • Frequency indicated by tick box • BGLs - relate to day of insulin administration • Hypoglycaemia section- extra BGL and action columns, record episodes and treatment • NB: All hypoglycaemic episodes should be managed immediately & include assessment for clinical review and must be fully document in health care record
Once Only S/C Insulin • Specify date and time dose to be administered • Nursing staff must initial and record time insulin administered
Telephone Orders • As per NSW Health policy • Refer to local policies • Signed within 24 hrs by MO
Page 4 • Guidelines for: • Management of hypoglycaemia • Management of hyperglycaemia • Use of supplemental insulin and correction of hyperglycaemia • For areas without local guidelines, policy or specialist support • Don’t take the place of local guidelines or policy
Acknowledgements • Inpatient Management Working Group • The many clinicians who have contributed to development and pilot of the Subcutaneous Insulin Medication Chart
ContactRebecca DonovanPH: 9464 4626Rebecca.Donovan@aci.health.nsw.gov.auMelissa Tinsley PH: 9464 4653melissa.tinsley@aci.health.nsw.gov.au .