Maternal Physiology in Pregnancy: Anatomical & Physiological Changes
320 likes | 476 Vues
Explore the intricate changes in cardiovascular, reproductive, respiratory systems, and mechanical adaptations during pregnancy. Understand the physiological mechanisms and implications for maternal health.

Maternal Physiology in Pregnancy: Anatomical & Physiological Changes
E N D
Presentation Transcript
Outlines • Introduction • Cardiovascular System changes • Reproductive System changes • Respiratory System changes • Mechanical changes
Introduction • Early changes: are due to • Metabolic demands of fetus, placenta, uterus • Increased level of pregnancy hormones (estrogen and progesterone). • Later changes: starting in mid-pregnancy, caused by mechanical pressure from the growing uterus.
System Organs Studied 1. Cardiovascular system 2. Reproductive organs 3. Respiratory system 4. Mechanical changes
1- Cardiovascular System • Blood volume • Blood constituents • Cardiac out put (COP) • Blood pressure (BP)
A. Blood volume • Increased progressively from 6 – 8 weeks gestation • Reach maximum at 32-34 weeks • Causes: • Increased capacity of the uterine, breast, renal, striated muscles, and cutaneous vascular system.
A. Blood volume (continue) • Plasma volume increased 40 – 50% • Red cell mass increase (20 – 30%) resulting in hemodilutionand decrease in hemoglobin concentration. • Intake of supplemental iron and folic acid is necessary to restore hemoglobin level to normal (12 g/dl).
A. Blood volume (continue) • Purposes: • It facilitates maternal and fetal exchanges of respiratory gases, nutrients, and metabolites. • It decreases the impact of maternal blood loss at delivery. • Normal labor 300-500 ml • CS: 750- 1000 ml • Auto-transfusion of blood from the contracting uterus.
B. Blood constituents • RBCs mass increases 20-30%. • Leukocytes remain within the upper limits of normal. increase after birth. • Clotting factors & fibrinogen: increased markedly.
B. Blood constituents • Blood platelets increased (within normal) • Fibrinolytic activity: decreased • These changes tend to prevent excessive bleeding at delivery.
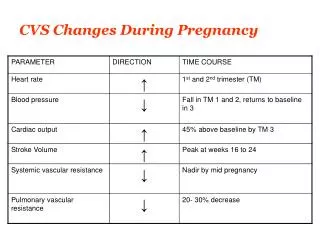
C. Cardiac output • Increases 30-40% during the 1st trimester. • Increases from an average of 6.7 L/ m at 8-11 weeks to about 8.7 L / m at 36-39 weeks; • This increase is due to • Increase in stroke volume (35%) • Rapid heart rate (15%).
D. blood pressure • ABP decreases toward the end of the 1st trimester • Because of: • Decrease in systemic vascular resistance • Decrease in peripheral vascular tone.
Supine Hypotension vana cava syndrome • Maternal position has an effect on BP when the uterus compresses the inferior vena cava, this occurs when the mother is in lying position (supine) and disappears in the left side lying position. • Occurs in 3 – 11% of pregnant women.
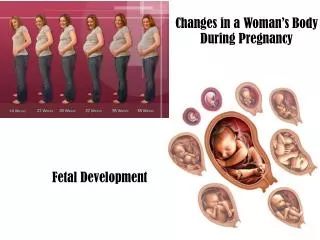
2- Reproductive System • The changes occur in the reproductive organs during pregnancy include uterus, cervix, and vagina. • These changes can be summarized in the following table:
Notes • Increased uterine size is due to: • Growing fetus, • ↑ in connective tissue • ↑ in the size and number of blood vessels to it.
Notes • The cervix, during labor, becomes shorter (effaces) and wider (dilates), effectively disappears. • If the cervix begins dilating prematurely, it is sometimes stitched together during the 2nd trimester, until fetal maturity, this procedure called "cerclage".
3- Respiratory System • Hyperventilation due to high level of progesterone. • Breathing pattern: becomes more costal than abdominal and most women are mouth breathers during pregnancy. • Anatomically: the diaphragm is in the higher position due to: • Expansion and elevation of the rib cage • Growing uterus at the late pregnancy.
a. Center of Gravity • COG shifts upwards and forwards due to the enlargement of the uterus and breasts.
b. Posture • Kyphosis & rounded shoulders: due to breast enlargement and post-partum positioning for infant care. • Cervical lordosis: and forward head posture. • Lumbar lordosis: increases to compensate for the shift of the COG and • Back-knee: knee hyper-extended.
b. Posture (continued) • Weight shifts: towards the heels. • Systemic hyper-laxity: due to increase in the level of relaxin hormone. • Mechanical back pain: due to weakness of abdominals, and strain of back muscles
c. Balance • Due to increase in weight and redistribution of body mass, the following occurs: • Waddling gait: to increase stability as the BOS increased. • Difficulties in some activities such as walking, stooping, stair climbing, lifting.