Download
1 / 24
240 likes | 261 Vues
This study examines the relationship-based quality of care in home health aide agencies with various ownership types. It delves into caregiver and client outcomes, productivity, and the concept of "Quality of Care."

E N D
Examining a Relationship-based Quality of Care in Organizations with Different Ownership Types Daphne P. Berry PhD Candidate University of Massachusetts Amherst Jan. 25, 2011
Agenda • Background and description of my exploratory dissertation study • Research methods and data • Some preliminary findings • Contributions and future research
This study is about… • Ownership and participation in home health aide agency sector • Home Health Aide (HHA) agency outcomes to caregivers (job satisfaction, org. commitment) and clients • Productivity and a specific conceptualization of “Quality of Care”
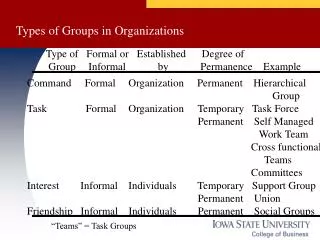
Home Health Organization Types http://leadingage.org/about.aspx
Concepts Defining quality in a Quality system Medical setting Direct care (includes nursing homes) setting Home health care setting (Deming, 1982; Parasuraman, Zeithaml and Berry, 1985; Donabedian, 2005; Mor, 2006; Eaton, 2000)
Concepts Caring labor Usually worker and recipient in close contact. Involves “caring for” and “caring about” the recipient. Depends on the relationship between a caregiver and the person cared for. Often, it is done for low or no pay. (Folbre, 2003, 2001; Badgett and Folbre, 1999; Himmelweit, 1999)
Home Health Aides Assist people with disabilities, are chronically ill, cognitively impaired and elderly to live in their own homes. • Must obtain and maintain certification from states, Knowledgeable about host of medical conditions, medications. • Perform light housekeeping. • Assist clients in and out of bed, with bathing, dressing, toileting, grooming. • Provide basic health-related services: checking pulse rate, temperature, and respiration rate; help with simple prescribed exercises; assist with medications administration; change simple dressings; give massages, provide skin care; or assist with braces and artificial limbs; assist with medical equipment such as ventilators. • Accompany to appointments.
federal and state programs care coordinators care coordinators care coordinators agencies agencies agencies agencies direct service workers and clients direct service workers and clients direct service workers and clients direct service workers and clients Home Health Aide Agency Environment federal and state programs federal and state programs care coordinators agencies direct service workers and clients (*From Scala, 2008) Home and Community Based Services: (Workforce and Quality Outcomes)
Quality Care • Clinical aspects • In home health environment, process measures are often counts of • How often home health team determined whether patients had received a flu shot or • Tasks to be completed by someone other than the HHA (e.g. pain or depression assessment conducted) • Heavy reliance on outcome indicators: improvement or stabilization in • Discharge to community, acute care hospitalization • Patient ability to transfer to and from bed, groom, dress, manage medications; Home care team checked or cared for ulcers, wounds, UTIs, etc. www.medicare.gov/HomeHealthCompare/Data/Measures/List.aspx
Quality Care Relationship between caregivers and clients is important Respect Security Caring Reliability (Mor, 2006; Eaton, 2000)
Multi-method data collection Qualitative Interviews – with home health aides, coordinators and other agency management (24) Observations – during internal meetings, training sessions (approx. 30) Documents – internal agency and publicly-available (50+) Quantitative Survey (628 respondents total from 3 agencies)
Research Process • Interviews and observation for data on organizational processes, for use with survey regarding quality of care items. • Use items from pre-validated measure*, items from interviews, home health aides and staff participated in validation of final survey** *survey instrument from “Shared Capitalism” research (Kruse, Freeman, Blasi, 2010) ** survey provided in English and Spanish
Initial propositions How workers with or without an ownership stake in the business and involved in organizational decision-making would respond related to: • quality of care to clients • levels of job satisfaction • relations with management
Multiple comparisons, ANOVA means plots, organizations not significantly different OrgType- 1: For Profit, 2: Non Profit, 3: Worker Cooperative
Multiple comparisons, ANOVA means plots, Worker Coop different from others OrgType- 1: For Profit, 2: Non Profit, 3: Worker Cooperative
Multiple comparisons, ANOVA means plots, All organizations different OrgType- 1: For Profit, 2: Non Profit, 3: Worker Cooperative
Qualitative data From caregivers at the cooperative: • “The cooperative is a great place to work.” • “Providing quality care is having the right training, caring about patients.” • “Taking care of patients is a hard job. I believe we should make $10 an hour for the work we have to do in a patient’s home. We aides go through a lot...” From the for-profit: • “Hell no I don't get paid fairly for what I do.” • “We need more pay… we work like slaves for little pay.” • “HHAs are not treated with any respect by the coordinator and others in the office. They speak in a condescending manner, very impatient and don't listen very well to HHAs but they expect to be given respect… (Company) needs to be investigated for abuse of labor and poor wages.”
Qualitative data From the non-profit: • “I enjoy caring for people. People in the administration have always been kind but we should get paid more.” • “Some of the HHAs receive bad treatment from the clients or the client's family members -disrespect, cruel words, etc. We can request to be removed but sometimes there might not be a vacancy for a while. And even though the salary is small, some of us stay because we are not sure if we will get a worse case or an immediate vacancy. Of course, there are wonderful clients and family members as well. I have a college degree (associates). I was thinking to become a nurse. I wanted a job and to see what it was like to work in the home and help people. Soon, I will move on…”
Preliminary findings • For quality of care – participation related to HHA decision-making is important. • For job satisfaction – organization type not most important, participation related to HHA decision-making, inclusion and sharing are important. • For management-employee relations – organization type and participation related to decision-making, inclusion and sharing are important.
Conclusion • Even in an industry with such challenging staffing and other problems as home care, employee participation in workplace decisions is associated with positive outcomes for workers, businesses and clients.
Contributions • Under-researched industry: home care and the work environment of a critically-needed segment of workers • Adding to the initial studies related to quality of care: focus on caregiver – client relationship, intertwined outcomes to clients and caregivers • Attention to democratic workplaces in the form of worker-owned organizations, associated participatory decision making
Future research • In the home health aide industry • Further development of relationship-based quality of care measure • Study of how structural environment - including extensive monitoring - may affect quality of care provided • Expanded study of quality of care concept including perspectives of clients • Study of how participation in decision-making impacts more comprehensive set of outcomes for the caregivers
Thank you. Questions?