Download
1 / 62
650 likes | 824 Vues
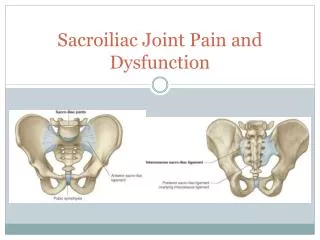
Sacroiliac Joint Pain, A Review. Ahmad Al-khayer SpR Rehabilitation Medicine. Controversies. Anatomy SIJ movements Do clinical tests have a role? Is imaging conclusive? Is SIJ intraarticular injection conclusive? Treatment??. Controversies. Anatomy SIJ movements

E N D
Sacroiliac Joint Pain, A Review Ahmad Al-khayer SpR Rehabilitation Medicine
Controversies • Anatomy • SIJ movements • Do clinical tests have a role? • Is imaging conclusive? • Is SIJ intraarticular injection conclusive? • Treatment??
Controversies • Anatomy • SIJ movements • Do clinical tests have a role? • Is imaging conclusive? • Is SIJ intraarticular injection conclusive? • Treatment?? • The diagnosis of SIJ pain is in itself controversial!!!
Aims • History • Anatomy, Biomechanics, Movements • Pathophysiology • Diagnosis (Pain Distributions, Clinical & Radiological Tests, Intraarticular injection) • Treatment (Conservative, Minimally Invasive, Surgical)
History • Hippocrates observed that a woman’s pelvis separated during labour and remained so after birth. Lynch 1920 (Surg Gynecol Obstet 575-580)
History • Hippocrates observed that a woman’s pelvis separated during labour and remained so after birth. Lynch 1920 (Surg Gynecol Obstet 575-580) • Albee 1909 (JAMA 53;1273-67), Smith-Paterson 1926 (JBJS 8;118-136), Campbell 1927(Surg Gynecol Obstet 45;218-9)
History • Hippocrates observed that a woman’s pelvis separated during labour and remained so after birth. Lynch 1920 (Surg Gynecol Obstet 575-580) • Albee 1909 (JAMA 53;1273-67), Smith-Paterson 1926 (JBJS 8;118-136), Campbell 1927(Surg Gynecol Obstet 45;218-9) • Development of discectomy surgery by Mixter and Barr 1934 (New Engl J Med 211;210-15)
History • Hippocrates observed that a woman’s pelvis separated during labour and remained so after birth. Lynch 1920 (Surg Gynecol Obstet 575-580) • Albee 1909 (JAMA 53;1273-67), Smith-Paterson 1926 (JBJS 8;118-136), Campbell 1927(Surg Gynecol Obstet 45;218-9) • Development of discectomy surgery by Mixter and Barr 1934 (New Engl J Med 211;210-15) • Schwarzer 1995 (Spine 20;31-7), Maigne 1996 (Spine 21:1889-92), Katz 2003 (J Spinal Disord Tech 16;96-9). The cause of chronic low back pain in 13-30% of patients.
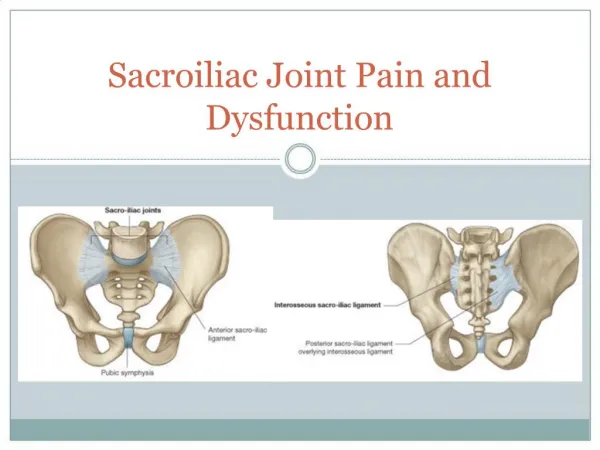
C or Ear shaped by adulthood. Fibrous capsule; thin anteriorly, absent posteriorly Synovial (75% of its superior part is not) Anatomy
C or Ear shaped Fibrous capsule; thin anteriorly, absent posteriorly Synovial (75% of its superior part is not) True diarthrodial joint: The concave sacral surface is covered with thick hyaline cartilage, the convex iliac surface is covered with fibrocartilage Anatomy
Ant Post Anatomy
The morphology of the SIJ changes with age; Flat until puberty By 30 bony ridges on the ilium side By fourth decade ridges on both sides Anatomy
The morphology of the SIJ changes with age; Flat until puberty By 30 bony ridges on the ilium side By fourth decade ridges on both sides Anatomy • It varies greatly in size, shape, contour from side to side and between individuals
The morphology of the SIJ changes with age; Flat until puberty By 30 bony ridges on the ilium side By fourth decade ridges on both sides Anatomy • It varies greatly in size, shape, contour from side to side and between individuals • The synovial cleft narrows with age; 1-2mm in individuals aged 50 to 70 0-1mm in over 70
The old bridge of Stirling, built about 1550 • Both Highland troops and the British army tried to cross during the 1745 Jacobite rebellion
Biomechanics • “Keystone in an arch”effect; the greater the force the greater the resistance
Biomechanics • “Keystone in an arch”effect; the greater the force the greater the resistance • Triplanar shock absorber, base of spine • Transmits and dissipates upper trunk loads
Movements • Powerful ligament (interosseous) • Different and variable shape • Keystone
Movements • Powerful ligament (interosseous) • Different and variable shape • Keystone Does it actually move?
Movements • Many type of movements have been described by Weisl 1955, Mitchell 1979, Beal 1982, Woerman 1982, Aitken 1986, Bernard 1987, Lee 1989, Shaw 1992, Oldrieve 1996)
Movements • Many type of movements have been described by Weisl 1955, Mitchell 1979, Beal 1982, Woerman 1982, Aitken 1986, Bernard 1987, Lee 1989, Shaw 1992, Oldrieve 1996) • Movement of ilium on the sacrum (upslip, downslip, outflare, inflare, anterior torsion, posterior torsion) • Movement of sacrum on the ilium (nutation, counter-nutation, sacral side bending, rotation)
Movements • “Movements of the sacroiliac joints. A roentgen stereophotogrammetric analysis”. Sturessone et al 1989, (Spine 14(2): 162-5) • 25 patients (21F: 4M). Physiological and extreme physiological positions. Mean rotations around axial axis 2.5 degrees (0.8 degree-3.9 degrees). Mean translation was 0.7 mm (0.1-1.6 mm).
Movements • The two most common types of motion are nutation (backward rotation of the ilium on the sacrum) and counternutation (forward rotation) • SIJ motion progressivelydecreases in men aged between 40 and 50 and in women aged over 50. Dreyfuss 1995 (Spine 6;785-813)
Pathophysiology • Multiple theories: • Ligamentous or Capsular tension • Bony arthritis • Synovial inflammation • Extraneous compression or shear forces • Hypo or hypermobility • Abnormal mechanics • Myofascial
Pathophysiology • SIJ dysfunction (postpartum, limb length discrepancy, repetitive minor trauma) • Infection (haematogenous) • Spondyloarthropathies (Ank spond, Reiter’s) • Degenerative arthritis • Post traumatic arthritis (insufficiency factures, major trauma) • Previous spinal surgery (lumbar stabilisation....)
Pathophysiology (less frequent) • Metabolic and endocrine disorders (crystal induced joint disorders, hyperparathyroidism) • Primary tumors (chondrosarcoma, giant cell tumors...) • Mets to pelvis • Idiopathic • Rare causes (iatrogenic, psychogenic).
Pathophysiology • Dreyfuss 1995 (Clin N Am 6;785-813) • Intraarticular sources: Spondyloarthropathies, OA, infection, metabolic • Extraarticular sources: ligamentous sprain, SIJ fractures, insufficiency fractures, ligamentous, tendious, fascial attachment • Tumors • Iatrogenic
Pathophysiology • Dreyfuss 1995 (Clin N Am 6;785-813) • Intraarticular sources: Spondyloarthropathies, OA, infection, metabolic • Extraarticular sources: ligamentous sprain, SIJ fractures, insufficiency fractures, ligamentous, tedious, fascial attachment • Tumors • Iatrogenic • Could the above be relevant for treatment?
Diagnosis Pain distribution Clinical Tests Radiological Investigations Intraarticular Injection
Pain Distributions • Fortin et al 1994 (Spine;19:1475-82). 10 asymptomatic volunteers, SIJ injection with contrast material followed by Xylocaine. Buttock hypoesthesia extending approximately 10 cm caudally and 3 cm laterally from the posterior superior iliac spine. This corresponded to the area of maximal pain noted upon injection. SIJ pain referral map was generated.
Pain Distributions • Fortin et al 1994 (Spine;19:1483-9). 54 patients completed pain diagrams. Two blinded clinicians selected 16 patients whose diagrams most represented the SIJ referral diagrams from study 1. 100% of these 16 had pain provocation with SIJ injection.
Pain Distributions • Fortin et al 1994 (Spine;19:1483-9). 54 patients completed pain diagrams. Two blinded clinicians selected 16 patients whose diagrams most represented the SIJ referral diagrams from study 1. 100% of these 16 had pain provocation with SIJ injection. How many of the remaining could have had SIJ pain too?
Pain Distributions • Slipman et al 2000 (Arch Phys Med Rehabil 81;334-8) 50 (18M:32F) patients. All demonstrated a positive diagnostic response to a fluoroscopically guided SIJ injection. Each patient's preinjection pain description was used to determine areas of pain referral.
Pain Distributions • Slipman et al 2000 (Arch Phys Med Rehabil 81;334-8) 50 (18M:32F) patients. All demonstrated a positive diagnostic response to a fluoroscopically guided SIJ injection. Each patient's preinjection pain description was used to determine areas of pain referral. 47 buttock pain, 36 lower lumbar pain. 7 groin pain. 25 lower-extremity pain. 14 leg pain distal to the knee, and 6 patients reported foot pain.
Pain Distributions • Slipman et al 2000 (Arch Phys Med Rehabil 81;334-8) 50 (18M:32F) patients. All demonstrated a positive diagnostic response to a fluoroscopically guided SIJ injection. Each patient's preinjection pain description was used to determine areas of pain referral. 47 buttock pain, 36 lower lumbar pain. 7 groin pain. 25 lower-extremity pain. 14 leg pain distal to the knee, and 6 patients reported foot pain. 18 potential pain-referral zones were established.
Pain Distributions Only 4% of patients mark any pain above L5 on self reported Pain drawings. Dreyfuss 1996 (Spine, 21:2594-2602)
Pain Distributions Many diseases mimic SIJ pain: Spinal disorders Non- spinal disorders: Gastrointestinal Genitourinary Pubic symphysis motion Myofascial imbalances Aberrant gait Hip joint disorders
Clinical Tests • Pain provocative tests • Palpation tests • Motion demands tests
Clinical Tests • Pain provocative tests • Patrick’s test 77% sensitivity, 100 % specificity*. (FABER) • Thigh thrust test 80% sensitivity, 100% specificity*. (Post shearing stress applied to SIJ through Femur) • * (Broadhurst 1998, J Spinal Disord 11;341-345) • Palpation tests • Motion demands tests
Clinical Tests • Pain provocative tests • Palpation tests • The midline sacral thrust test 89% sensitivity, 14% specificity (patient prone, post ant force) • (Dreyfuss 1996 Spine 21:2594-2602) • Motion demands tests
Clinical Tests • Pain provocative tests • Palpation tests • Motion demands tests Sitting tolerance 78% sensitivity, 58% specificity (Stark et al) Standing, Flexion
Clinical Tests Partick’s test Yeaoman’s test Lewin Ganslen’ test Pelvic rock’ test Stretch test
Clinical Tests • Clinical examination cannot definitely confirm that the SIJ is the source of patient’s pain *Dreyfuss P et al; Spine 1996; 21(22): 2594–602. Van der Wurff P et al ; Man Ther, 2000; 5(1): 30-6. Van der Wurff P et al ; Man Ther, 2000; 5(2): 89-96*
Radiological Investigations • X-rays, CT, MRI, and bone scan do not provide consistent findings that can be used for the diagnosis *Prather H; Clin J Sport Med, 2003; 13(4): 252-5, Dreyfuss P et al; Am Acad Orthop Surg. 2004; 12(4):255-65, Rothschild BM et al; Clin Exp Rheumatol, 1994; 12(3): 267-74*
Intraarticular Injection • LA • Gold standard for diagnosis of intraarticular SIJ pain • 70-80% relief of pain is diagnostic *Dreyfuss P et al; Am Acad Orthop Surg. 2004; 12(4):255-65, Maldjian C et al; Radiol Clin North Am, 1998; 36(3): 497-508. Maigne JY et al; Spine, 1996; 21(16): 1889-92. Luukkainen RK et al; Clin Exp Rheumatol. 2002; 20(1):52-4*
Intraarticular InjectionThe Technique • Dussault et al 2000(Radiology, 214:273-7) Patients prone. C-arm fluoroscope angled 20 to 25 in a caudal direction. Straight needle is advanced perpendicular to the table aiming to post inf part of SIJ. 97% success rate reported.