Download
1 / 57
570 likes | 823 Vues
Kimi Watkins-Tartt Director of Community Health Services Alameda County Public Health Department Transforming Systems: Achieving Health Equity October 14, 2011. Transforming Public Health Practice: Social and Health Equity in Alameda County. Acknowledgements.

E N D
Kimi Watkins-Tartt Director of Community Health Services Alameda County Public Health Department Transforming Systems: Achieving Health Equity October 14, 2011 Transforming Public Health Practice: Social and Health Equity in Alameda County
Acknowledgements The information presented in this presentation represents the ideas , hard work, and expertise of many Alameda County Public Health Department Staff, partners, and community members.
Why focus on achieving health equity in Alameda County? What were the key components of developing our Strategic Plan? Howare we working towards health equity? How are we implementing our Strategic Plan? What does it take? What’snext? Overview
Our Mission To work in partnership with the community to ensure the optimal health and well being of ALL people through a dynamic and responsive process respecting the diversity of the community and challenging us to provide for present and future generations. Why do we focus on health equity?
Place Matters: Health Inequities by Where People Live
Income Matters:Health Inequities by Neighborhood Poverty In 1999, the federal poverty level was $8,500 for one person living alone and $17,000 for a family of four.
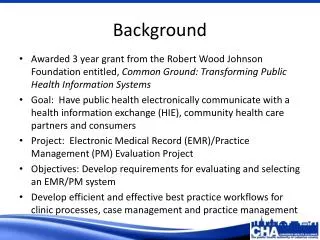
7.8 years 4.9 years 2.3 years Race and Racism Matters:Health Inequities by Race/Ethnicity
1.5 times more likely to be born premature or low birth weight 2.5 times more likely to be behind in vaccinations 5 times more likelyto be hospitalized for diabetes 7 times more likely to be born into poverty 4 times less likely to read at grade level 2 times more likely to die of heart disease Cumulative impact: 15 year difference in life expectancy Racism, Place, and Income impact health Compared to a White child in the affluent Oakland Hills, an African American born in West Oakland is… INFANT CHILD ADULT
Health Inequities Health inequities are “differences in health which are not only unnecessary and avoidable but, in addition, are considered unfair and unjust.” -Margaret Whitehead Department of Public Health University of Liverpool
Why have health benefits not been experienced equally across population groups?
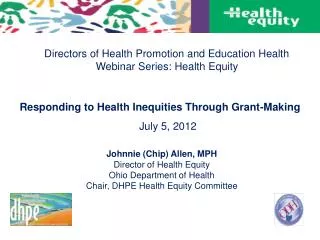
A Framework for Health Equity A Framework for Health Equity Socio-Ecological Medical Model A Framework for Health Equity Socio-Ecological Medical Model A Framework for Health Equity Socio-Ecological Medical Model Socio-Ecological Medical Model INDIVIDUAL HEALTH KNOWLEDGE INDIVIDUAL HEALTH KNOWLEDGE INDIVIDUAL HEALTH KNOWLEDGE GENETICS INDIVIDUAL HEALTH KNOWLEDGE GENETICS Upstream Downstream GENETICS Upstream Downstream GENETICS Upstream Downstream Upstream Downstream • Discriminatory • Beliefs (Isms) • Race • Class • Gender • Immigration status • National origin • Sexual • orientation • Disability • Institutional Power • Corporations & other businesses • Government agencies • Schools • Social • Inequities • Neighborhood conditions • - Social • - Physical • Residential segregation • Workplace conditions • Risk Factors & • Behaviors • Smoking • Nutrition • Physical • activity • Violence • Chronic Stress • Disease • & Injury • Infectious • disease • Chronic • disease • Injury (intentional & unintentional) • Mortality • Infant • mortality • Life • expectancy • Discriminatory • Beliefs (Isms) • Race • Class • Gender • Immigration status • National origin • Sexual • orientation • Disability • Institutional Power • Corporations & other businesses • Government agencies • Schools • Social • Inequities • Neighborhood conditions • - Social • - Physical • Residential segregation • Workplace conditions • Risk Factors & • Behaviors • Smoking • Nutrition • Physical • activity • Violence • Chronic Stress • Disease • & Injury • Infectious • disease • Chronic • disease • Injury (intentional & unintentional) • Mortality • Infant • mortality • Life • expectancy • Discriminatory • Beliefs (Isms) • Race • Class • Gender • Immigration status • National origin • Sexual • orientation • Disability • Institutional Power • Corporations & other businesses • Government agencies • Schools • Social • Inequities • Neighborhood conditions • - Social • - Physical • Residential segregation • Workplace conditions • Risk Factors & • Behaviors • Smoking • Nutrition • Physical • activity • Violence • Chronic Stress • Disease • & Injury • Infectious • disease • Chronic • disease • Injury (intentional & unintentional) • Mortality • Infant • mortality • Life • expectancy • Discriminatory • Beliefs (Isms) • Race • Class • Gender • Immigration status • National origin • Sexual • orientation • Disability • Institutional Power • Corporations & other businesses • Government agencies • Schools • Social • Inequities • Neighborhood conditions • - Social • - Physical • Residential segregation • Workplace conditions • Risk Factors & • Behaviors • Smoking • Nutrition • Physical • activity • Violence • Chronic Stress • Disease • & Injury • Infectious • disease • Chronic • disease • Injury (intentional & unintentional) • Mortality • Infant • mortality • Life • expectancy HEALTH STATUS HEALTHCARE ACCESS HEALTH STATUS SOCIAL FACTORS HEALTHCARE ACCESS HEALTH STATUS SOCIAL FACTORS HEALTHCARE ACCESS HEALTH STATUS SOCIAL FACTORS HEALTHCARE ACCESS SOCIAL FACTORS - Adapted by ACPHD from the Bay Area Regional Health Inequities Initiative, Summer 2008 - Adapted by ACPHD from the Bay Area Regional Health Inequities Initiative, Summer 2008
When the External Becomes Internal How Health Inequities Get Inside the Body Physical and Mental Health Impacts Increased commute times Transportation Stress Stress Lack of access to stores, jobs, services Poor air quality Stress Stress Segregation Stress Stress Crime Housing Stress Poor quality Education Stress
Health Equity Everyone in Alameda County, no matter where you live, how much money you make, or the color of your skin, has access to the same opportunities to lead a healthy, fulfilling and productive life.
Policy & Systems Change Programs Services HEALTH EQUITY Community Collaborations & Partnerships Institutional Change Data and Research ACPHD’s Approach to Achieving Health Equity
ACPHD’s Approach to Achieving Health Equity Policy & Systems Change Programs Services HEALTH EQUITY Community Collaborations & Partnerships Institutional Change Data and Research
Community Capacity Building: Community Identified Projects Sobrante Park • Improve Tyrone Carney Park/streetscape • Reduce drug dealing and violence • Create more positive activities for youth • Prepare the neighborhood for disasters West Oakland • Renovate Durant Park • Reduce blight • Create a continuum of improved and connected youth services & employment
Successes: Community Capacity Building Meaningful opportunities for participation Civic participation “Social Capital” Improved built environment Emergency preparedness Cleanliness Community deterioration Blight Lower crime (in SP)
ACPHD’s Approach to Achieving Health Equity Policy & Systems Change Programs Services HEALTH EQUITY Community Collaborations & Partnerships Institutional Change Data and Research
Local Policy Agenda The Alameda County Place Matters team promotes health equity through a community-centered local policy agenda focused on education, economics, criminal justice, housing, land use, and transportation. place matters community engagement | criminal justice| economics| education | housing | land use + transportation
ACPHD’s Approach to Achieving Health Equity Policy & Systems Change Programs Services HEALTH EQUITY Community Collaborations & Partnerships Institutional Change Data and Research
What were the key components of developing our Strategic Plan? • Key principals • Our goal is achieving health equity • Our methodsare participatory—all voices are needed for a strong plan • Our approach is grounded in the principals of social justice • Our implementation will only be successful with widespread ownership of and support for the strategic plan
Internal and external participation Leadership Fellows CBOs & other Partners Community Residents Strategic Planning Process Public Health Department staff Public Health Commission Management Fellows Leadership Team
Internal Participation • Social Justice Dialogues and Group Discussions • Institutional Racism, Gender & Class Exploitation • SWOT analysis and recommendations • All-Staff Survey • Vision • Analysis of Strength, Weaknesses Opportunities and Threats (SWOT) • Recommendations • Completed by 340 staff (about 57%)
6 forums in 5 supervisorial districts (237 participants) • 1 forum in Spanish (44 participants) • Key Informant Interviews (10 with Board of Supervisors and agency directors) • Youth retreat External Participation
ACPHD Strategic Plan for Health Equity Transform our organizational culture and align our daily work to achieve health equity. Enhance Public Health communications internally and externally [to achieve health equity]. Ensure organizational accountability through measurable outcomes and community involvement. Support the development of a productive, creative, and accountable workforce. Advocate for policies that address social conditions impacting health. Cultivate and expand partnerships that are community-driven and innovative.
Howare we implementing our Strategic Plan? Cross-Departmental Workgroups Divisions
Hypothetical Example: Divisional Work Plan What we already have • Divisional Work Plan for CHS • Goal 1.1: Incorporate principles of social justice into public health activities. • CHS Objective: By end of fiscal year 2009-2010, CHS will develop criteria to ensure contractors are addressing health inequities. • Alcohol and Drug Program Objective: By the end of fiscal year 2009-2010, all contractors will participate in 3 trainings (institutional racism, health equity, and policy). • Alcohol and Drug Program Objective: By the end of fiscal year 2010-2011, all contracts will contain language that ensures contractors are meeting CHS Health Equity criteria. Strategic Direction 1: Transform our organizational culture and align our daily work to achieve health equity. What divisions are working on
Public Health 101 • ACPHD Internal Trainings and Staff Support: • Strategic Planning process & implementation • All-staff meeting: speakers, spoken word, films • BBUs • Unnatural Causes screenings Module 1: History of Public Health & the Public Health System Module 2: Cultural Competency and Cultural Humility Module 3: Undoing Racism Leadership and Management Fellows Module 4: Social and Health Equity Module 5: Community Capacity Building Staff Capacity: Root Causes of Health Inequities
Isms • Strategic Direction 1: Transform our organizational culture and align our daily work to achieve health equity • Goal 3: Expand staff understand of “isms” and health equity. • Internal Isms Trainings and Staff Support: • PH 101 Module 3 • Place Matters Orientation • BBUs • Leadership and Management Fellows • Strategic Planning Institutional Racism Discussions • CAPE Institutional Racism Discussions • Workshop with Dr. Kenneth Hardy Dr. Camara Jones Dr. Kenneth Hardy Photos: www.pbs.org/race www.unnaturalcauses.com www.psychotherapy.net/interview/Kenneth_Hardy
What’s next? • Quarterly Leadership Team oversight meetings to guide cross-departmental and division work • Tracking and evaluation of activities • Alignment with the HCSA Convergence process
ACPHD’s Approach to Achieving Health Equity Policy & Systems Change Programs Services HEALTH EQUITY Community Collaborations & Partnerships Institutional Change Data and Research
Programs & Services: Measure A Chronic Disease Prevention and/or Obesity Prevention Funding • Equity focused RFP including health inequity data • 2 info sessions focused on health equity • Call for socio-ecological solutions • Inclusive & transparent review panel • Support & feedback for those who didn’t receive the grant • Additional capacity building support is needed
ACPHD’s Approach to Achieving Health Equity Policy & Systems Change Programs Services HEALTH EQUITY Community Collaborations & Partnerships Institutional Change Data and Research
Success stories • Increased: • organizational infrastructure and support for health equity work, including addressing isms • support, commitment, participation, ownership • activities throughout the department & community • engagement in policy • Cutting-edge work • Community Engagement • Passionate Staff • Creativity • Setting a Model
What it Takes • Work with communities as partners • Constantly reflecton difficult issues • Createcommunication loops to hear positives and negatives • Involve and empower all levels of staff, which leads to ownership and progress • Stay focused on vision while breaking it into smaller steps • Engagediverse staff & supporthiring for diversity • Show long term commitment • Invest in building staff capacity and leadership • Address interpersonal and institutional “-isms” • Be open to conflict – it’s okay to be uncomfortable
What it takes What questions are we asking? How do these questions define the problem? How does the definition of the problem define the solution?
Why do people smoke? What social conditions and economic policies predispose people to the stress that encourages smoking? Flipping the Question DoakBloss, Ingham County Health Department
How can we create more green space, bike paths, and farmers’ markets in vulnerable neighborhoods? What policies and practices by government and commerce discourage access to transportation, recreational resources, and nutritious food in neighborhoods where health is poorest? Flipping the Question Doak Bloss, Ingham County Health Department
Flipping the Question/Solution • We need to teach people how to eat more healthful meals. What policies and practices by government, commerce, and corporations led to the decline of food stores in West Oakland?
Vision of Health Equity Everyone in Alameda County, no matter where you live, how much money you make, or the color of your skin, has access to the same opportunities to lead a healthy, fulfilling and productive life.
Policy Makers Childcare Medical Care Jobs Healthy Food We each have a role Clean Air Parks and Activities Housing Education Economic Justice Preschool Safe Neighbor-hoods Residents Transpor-tation
Contact information Kimi Watkins-Tartt Kimi.watkins-tartt@acgov.org510-208-5902
What Do We Know? • Major improvements in health outcomes • Major health inequities persist or are growing - poorer residents and African Americans bear the greatest burden of poor health outcomes • Big gap in life expectancy • Major inequities in life expectancy and mortality driven by chronic diseases
What Staff Capacity is needed to Address Health Inequities? Knowledge Skills Sensibilities • Policy analysis and advocacy • Using new tools and technology • Communication • Cultural competency • Community Capacity Building • Engaging partners and community • Root causes of health inequities • Isms: historical and current; and impact on health • Understanding our communities • Principles of social justice • Feeling empowered • Innovation • Cultural Humility Adapted from ACPHD Strategic Plan www.acphd.org/healthequity/strategic