Download
1 / 34
350 likes | 2.09k Vues
PELVIC GIRDLE PAIN (ALSO KNOWN AS SYMPHYSIS PUBIS DYSFUNCTION). The Gap Study VANDA K. WELLOCK & MARGARET A. CRICHTON. DEFINITION. Pelvic Girdle Pain (PGP) may be defined as an abnormal stretching of the pubic joint during pregnancy (Wellock 2002).

E N D
PELVIC GIRDLE PAIN (ALSO KNOWN AS SYMPHYSIS PUBIS DYSFUNCTION) The Gap Study VANDA K. WELLOCK & MARGARET A. CRICHTON
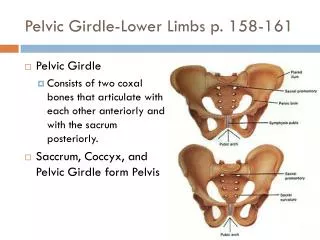
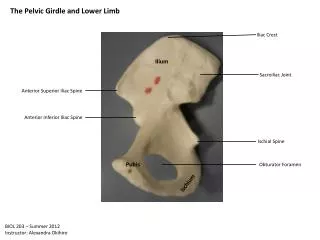
DEFINITION Pelvic Girdle Pain (PGP) may be defined as an abnormal stretching of the pubic joint during pregnancy (Wellock 2002). However more recently the ACPWH (2007) have described PGP/SPD as pain in the joints that make up the pelvic girdle and includes the symphysis pubis and/or the sacroiliac joints
Research proposal • Explore women’s understanding • Investigate women’s personal experience • Explore how women perceive their care from Health Care Professionals
Method & Design • Qualitative study using phenomenological approach to capture the “lived in experience” • Interviews at diagnosis, 36 weeks gestation and 6 weeks post partum
Sample & data Collection • Referred by Physiotherapy Department • Data collected over 15 month period • 28 women were recruited, no refusals or withdrawals. Total of 51 interviews for the study • 4 women interviewed three times, 14 twice and 11 once • Women interviewed in own homes
Themes • Women’s perception of pain and audible sounds • Interaction with Health Care Professionals • Gender roles within families
Women’s perception of Pain(1) The experience of pain was the most important finding in the study. Women do not expect, as a normal occurrence, pain in pregnancy. “my whole pelvis feels raw. I wish it was possible to apply a lubricant to the insides of my pelvis and bottom of my spine so that it wouldn’t grind…it’s the inside I wish I could reach” VM38
Pain “…I feel that I have a piece of wire…cheese wire, stuck around me...the groin area feels like somethings lodged there…” VM9 “…it felt raw, as if I was being sandpapered…all the muscles and everything…” VM11 “…all I remember is the bone area…I thought it was going to break…I couldn’t control the pain…I couldn’t hold it in …”VM47
Audible Sounds(1) It appears that the pain of PGP is a “noisy” pain. Different metaphors and similes were used by the women to describe the noise that emanated from the pelvic joints on mobilization. It seems it validated their pain experience. “ … so I’ve been getting a bit of crunching after my walks…I’ve been a bit sore…I hear a crunch, my partner has heard it…it’s like a crack…” VM25
Audible Sounds(2) “…I do hear funny sounds coming from inside me…it feels like it’s rubbing against things…it stops me in my tracks…it’s like a grind…it’s like something’s grinding like that…”VM 48 “…you can hear it clink, I’ve heard it clinking…my husband heard it too…it takes your breath away…”VM13
Interaction with Health Care Professionals The majority of women were satisfied with their care but felt there was room for improvement. “…Whatever has happened in that hospital has been brilliant…they were keyed up to the fact that that I had symphysis pubis dysfunction…”VM13
Interaction with Midwives “…midwives very supportive…usually they help you get up and they get you off (the couch) which way you think is best…” “…they all seemed really concerned…there wasn’t anything like “don’t worry about it, it’s just general aches and pains…I didn’t want to be a nuisance…”
Midwives cont. “…I saw the midwife at the surgery and she was trying to feel the baby and I was crying because it was hurting…she was feeling low down and it was really…really sore on symphysis pubis…”VM43 ”…I had to mention it to them…(midwives) even though it was on my notes (spd). To be honest it didn’t feel like they were taking an awful lot of notice of it…”VM2
Interaction with Doctors There appeared to be difficulty from the women in explaining the depth of the pain to doctors “…I went to the GP and explained about the pain and she said …”if you’re in that much pain why don’t you go to casualty?”…I was stuck inside all day…and I couldn’t move…and she said are you getting depressed? And I said well I am depressed that you’ve dragged me all the way here…the doctor was no good at all…” VM44
Doctors cont. Some women asked to be seen by a female doctor: “…male GP thought it was part of pregnancy (spd), the female doctor was more sympathetic…”VM38
Doctors cont. “…Consultant quite sympathetic towards (symphysis pubis dysfunction)…”VM20 “…A particular doctor was good, better than the midwives…”VM12
Doctors cont “…this doctor said ..”other than symphysis pubis dysfunction are you coping?..and something went inside me at the word “coping” and I screamed at him “if sitting on the kitchen floor at 3am with a knife in my hand and thinking…if I put a cut here, they will have to finish the job…and if that’s coping then I’m coping”..He had to find me someone to calm me down”…VM11
Midwives and Doctors during labour “…the midwife kept telling me to open my legs and my husband kept telling them “no she can’t”, he was trying to keep my legs together and they were trying to pull them further apart…”VM12 There appeared to be more interest in other conditions “…it’s more on the lines of …ehm…the rhesus antibodies side and it’s how you’re getting on with that…but it’s not affecting me and my SPD was…”VM32
Interaction with Physiotherapists “…think the world of (name of physio)…she gave advice…referred me to a pain clinic…and continues to be supportive” VM19 The long wait for an appointment to the department proved very distressing: “…she said she could put me down for it (appointment) but there would be no point…by the time it came through…there is a long wait for appointments….”VM30
Physiotherapists “…the physio was probably testing my physical limits, well I was in agony for two weeks…”VM44 “…what really annoys me more than anything really…is physios. You think the’ll do something but they can’t…”VM40
Pelvic Girdle Pain • Women with PGP experience great deal of pain, often exacerbated by movement • All of the activities of daily living caused pain and anxiety and affected their roles in life.
Domestic Role “…how do you cope?...it’s the one thing that is getting me down. The house is looking like a tip and I’m not house-proud or anything…but I like it dusted and I can’t do anything…”VM19 “…sometimes I can’t cook cos I can’t stand and do it and I’m putting things in the oven, bending down is very difficult…”VM38 I
Domestic role cont. “…It stopped me shopping, lifting, just everything really that I took for granted that I could do before…” VM6 Getting in and out of bed was a serious problem “…I wake in the morning and I can’t get up…I just lie there…I’ve had to ring my mum twice to come and get me up…and my little boy had been crying for me in his bedroom…I’ve had a few accidents waiting for her to come round…” VM17 “…I seem to have lost control over my life…”VM31
Maternal Role Many of the women had small children and not all had experience PGP before. This affected their ability to nurture their existing children and continue to do things with them “…couldn’t go to school to pick up the children, so I had to get taxis and everything…so it means I won’t be able to do anything with the children…” VM16
Maternal Role cont. Toilet training of the children and other aspects of childcare were affected. “…when she goes to the toilet (upstairs)…she would like a wash and she can’t because she needs me to help her…she was so good with toilet training and now it’s all gone…because I can only go up in an emergency because it’s so painful, I go up and down on my bottom…” VM3
Wife/Partner Role “…finally sorted out a bed in the spare room so I don’t have to sleep with my husband…I need all the room…because every time I turn over it’s a big ordeal…I wake him up and then if I did get comfortable and then he moved and made me move…we would have a big row and it was hard to get to sleep…” VM11
cont Maintaining some independence was also hard “…I’ve only got under bumper knickers…I’m not having my husband go in and buy them. I walked to the aisle and people were jostling and knocking me…I realised I could not make it…my husband gave me a pound for tea while he went shopping…I realised I couldn’t carry a tray and my crutches…no-one helped me…I burst into tears…I felt completely helpless…” VM38
Key findings • Women with PGP have a range of unmet needs • Most profound finding was the way the women’s rich narratives described their pain and the detrimental effects it had on their lives • Dissatisfaction with health care professionals arose when accounts of their “reality of pain” was rejected and they felt negatively labelled • Women became disabled by the condition. All the “taken for granted” activities of living were compromised and their lives made much more difficult. They felt guilty and frustrated about their loss of control
Implications for Practice • Raise awareness of effects of PGP by use of leaflets in all clinics • Provide guidelines and advertise them (available from Pelvic Partnership) • Training package for all staff in maternity units • Include topic in midwifery, nursing and medical training curriculums • More research to be undertaken
Practical Management • Discuss pain issues with women and their degree of pain and when it occurs it is often unpredictable and it responds to various coping strategies. • LSCS may not always be the answer.
Pain Management • Analgesia e.g Paracetamol • Physiotherapy /regular exercise • Pelvic support belts (the least effective belts are those mainly supplied in ante anatal clinics?) • Crutches and wheelchairs when mobility is impaired • Try alternative therapies e.g Bowen Technique, acupuncture, pilates, massage and heat • Body cushions/extra pillows in bed
Management • Make sure that PGP/SPD is clearly written on hand held notes and maternity records • Improve communication between midwives, physiotherapists and doctors • Seamless sharing of information between departments and all health care professionals • Fast track women with PGP to physiotherapy department for early help and support • Revision of Evidence Based protocols for women with PGP
Future Action As health care professionals we need to take action or we will continue to read articles such as those in “Take a Break” (August 2007) • Research a possible cause • Revision of pelvic support appliances with manufacturers in consultation with knowledgeable health care professionals • More research on alternative therapies • Encourage the setting up of local support groups • Dialogue with DVLA re mobility issues for women, especially with car parking • Benefit issues need exploring • Occupational health for equipment