Download
1 / 1
10 likes | 147 Vues
A Novel Approach to the Detection and Treatment of Raynaud’s Phenomenon: Using Non-invasive Methods. Danny Clegg 1 , Andrew Heusch 2 , Lee McCarthy 2 , Peter W McCarthy 1.

E N D
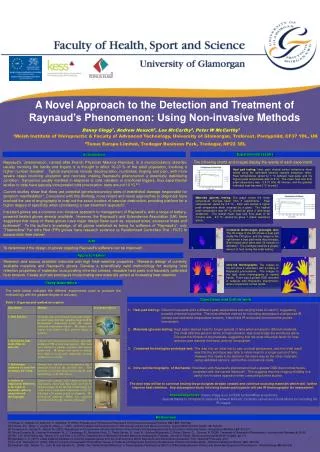
A Novel Approach to the Detection and Treatment of Raynaud’s Phenomenon: Using Non-invasive Methods Danny Clegg1, Andrew Heusch2, Lee McCarthy2, Peter W McCarthy1 1Welsh Institute of Chiropractic & Faculty of Advanced Technology, University of Glamorgan, Treforest, Pontypridd, CF37 1DL, UK 2Tonus Europe Limited, Tredegar Business Park, Tredegar, NP22 3EL Experimental results Introduction The following charts and images display the results of each experiment Raynaud’s phenomenon, named after French Physician Maurice Raynaud, is a microcirculatory disorder, usually involving the hands and fingers. It is thought to affect 10-20 % of the adult population, involving a higher number females1. Typical symptoms include discolouration, numbness, tingling and pain, with more severe cases involving ulceration and necrosis; making Raynaud’s phenomenon a potentially debilitating condition. Symptoms usually manifest in response to cold, vibration or emotional triggers, thus experimental studies to date have typically incorporated cold provocation tests around 10 oC 2,3. Current studies show that there are potential genetic/secondary sites of endothelial damage responsible for symptom manifestation4. Concurrent with this thinking, more recent and novel approaches to diagnosis have involved the use of angiography to map out the exact location of vascular destruction, providing platform for a higher degree of specificity when considering a new treatment approach5. Insulated gloves are a common non-invasive approach to management of Raynaud’s, with a range of battery-powered heated gloves already available. However, the Raynaud’s and Scleroderma Association (UK) have suggested that many of these gloves have major design flaws such as: exposed wires, excessive mass and bulkiness6. To the author’s knowledge, of all gloves marketed as being for sufferers of “Raynaud’s”, only “Thermoflow” Far Infra Red (FIR) gloves have research evidence (a Randomised Controlled Trial : RCT) to substantiate their claims7. To determine if the design of gloves targeting Raynaud’s sufferers can be improved. Research and source available materials with high heat-retentive properties. Research design of currently available materials and Raynaud’s gloves. Develop a scientifically valid methodology for studying heat retention properties of materials: incorporating infra-red camera, reusable heat pads and traceably calibrated heat sensors. Create and test prototypes incorporating new materials aimed at increasing heat-retention. Heat pad testing: Heat pads elicited similar behaviours when tested using the calibrated sensors (sample frequency 1kHz). Peak temperatures varied by 1 oC between heat pads, and the highest peak temperature was 41.9 oC. The mean heat loss from peak temperature was -3.8 oC after 45 minutes, and the greatest individual heat loss was 5 oC by pad 2. Materials (gloves) testing: The graph shows the mean temperature changes taken from 3 experiments. Peak temperatures varied by 3.5 oC. Each pad elicited a higher peak temperature when encased by a glove. The highest peak temperature was 45 oC, elicited by glove 2 (mid-range windproof). The lowest mean heat loss from peak to 45 minutes was -2.4 oC, elicited by glove 1 (basic wool/lycra glove). Combined technologies prototype test: The IR image to the left shows a heat pad inside the FIR glove, and the image to the right shows a heat pad inside the prototype. Both images were taken after 20 minutes of activation. The prototype retained a greater amount of heat during this initial testing. Aim Approach taken infra-red thermography: The images to the left show 2 volunteers with a history of Raynaud’s phenomenon. The images to the right show thermographs of normal hands. There was a greater DDD recorded in subjects with Raynaud’s phenomenon when compared to normal hands. Study description The table below indicates the different experiments used to produce the methodology with the greatest degree of accuracy. Table 1: Experimental method description Conclusion and further work • Heat pad testing: Different heat pads elicit a different peak temperature and varying times to reach it, suggesting possible chemical impurities. The most effective method for recording temperature change was IR camera and calibrated temperature sensors. Hand-held IR and probe thermometers proved inconsistent. • Materials (gloves) testing: Heat pads retained heat for longer periods of time when encased in different materials. The most effective glove in terms of heat retention, was surprisingly the wool/lycra glove. This was the thickest of the materials, suggesting that the most influential factor for heat retention was material thickness, and not composition. • Combined technologies prototype test: This was only an initial test to gain a visual perspective, and the initial result was that the prototype was able to retain heat for a longer period of time. However this needs to be tested in the same way as the other materials, using calibrated sensors, and further conclusions made. • infra-red thermography of the hands: Volunteers with Raynaud’s phenomenon had a greater DDD than normal hands., consistent with the current literature8. This suggests that this imaging modality is a useful non-invasive approach when conducting further studies. • The next step will be to continue testing the prototypes already created and continue sourcing materials which will further improve heat retention. Any subsequent study involving human participants will use IR thermography for assessment. • Acknowledgements: Danny Clegg is on a KESS funded MRes programme • Special thanks to Chiropractic students Stewart Bennett, Elizabeth James and CinziaMonni for recording the IR images [1] Silman, A., Holligan, S., Brennan, P., Maddison P. (1990). Prevalence of Symptoms of Raynaud’s Phenomenon in General Practice. BMJ, 301: 590-592 [2] Pelmear, P.L., Roos, J., Leong, D., Wong, L. (1987). Cold Provocation Test Results from a 1985 Survey of Hard-rock Miners in Ontario. Scand J Work Environ Health,13: 343-347 [3] Thompson, A., House, R., Manno M. (2007). Assessment of the Hand-arm Vibration Syndrome: Thermometry, Plethysmography and the Stockholm Workshop Scale. Occupational Medicine,57: 512-517 [4] García-Carrasco M,, Jiménez-Hernández, M,, O. Escárcega, R,, Mendoza-Pinto, C,, Pardo-Santos, R., Levy, R,, Galarza Maldonado, C.,Pérez Chávez, G.,, Cervera, R. (2008). Treatment of Raynaud’s Phenomenon. Autoimmunity Reviews, 8: 62-68 [5] Kim, Y.H., Siew-Weng, Ng., Heung, S.S. and Hee, C.A. (2011). Classification of Raynaud’s Disease Based on Angiographic Findings. Journal of Plastic, Reconstructive and Aesthetic Surgery, xx: 1-9 [6] Mawdsley, A. H. (2011). Letter detailing feedback on currently available gloves from the chief executive off the Raynaud’s and Scleroderma Association (UK), dated 23rd February, 2011 [7] Ko, G.D., Berbrayer, D. (2002). Effect of Ceramic-Impregnated “Thermoflow” Gloves on Patients with Raynaud’s Syndrome: Randomized, Placebo-Controlled Study. Alternative Medicine Review, 7(4): 328-335 [8] Anderson, M.E., Moore, T.L., Lunt, M. And Herrick, A.L. (2006). The ‘Distal–Dorsal Difference’: a Thermographic Parameter by Which to Differentiate Between Primary and Secondary Raynaud’s Phenomenon. Rheumatology,46: 533-538 References