Phase II Study of S-1 Plus Leucovorin as First-Line Treatment for Metastatic Colorectal Cancer
This study explores the efficacy and safety of the oral fluoropyrimidine S-1 combined with oral leucovorin (LV) as a first-line treatment for untreated metastatic colorectal cancer (mCRC). A total of 65 patients were enrolled, receiving a recommended dose of S-1 (40-60 mg/body) with LV (25 mg/body) twice daily for 14 days of a 28-day cycle. Results indicated a promising objective response rate of 57% and favorable disease control rates, with manageable toxicities. The regimen shows potential as a well-tolerated treatment option, eliminating the need for oxaliplatin or irinotecan.

Phase II Study of S-1 Plus Leucovorin as First-Line Treatment for Metastatic Colorectal Cancer
E N D
Presentation Transcript
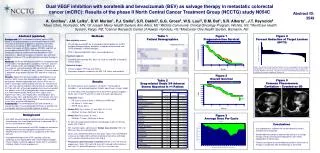
Phase I/II study of oral fluoropyrimidine S-1 plus oral Leucovorin as first-line treatment for metastatic colorectal cancer T. Yoshino1, W. Koizumi2, K. Yamaguchi3, Y. Miyata4, T. Kato5, Y. Toh6, A. Sawaki7, I. Hyodo8, T. Nishina9, N. Boku1 1Shizuoka Cancer Center, Shizuoka, JAPAN, 2Kitasato University East Hospital, Kanagawa, JAPAN, 3Saitama Cancer Center, Saitama, JAPAN, 4Saku Central Hospital, Nagano, JAPAN, 5Minoh City Hospital, Osaka, JAPAN, 6National Kyushu Cancer Center, Fukuoka, JAPAN, 7Aichi Cancer Center Hospital, Nagoya, JAPAN, 8University of Tsukuba, Tsukuba, JAPAN, 9NHO Shikoku Cancer Center, Matsuyama, JAPAN.
Updated Abstract Background:The results of phase I portion of the treatment with the oral S-1 (a new oral fluoropyrimidine) plus oral leucovorin (LV) in patients (pts) with untreated metastatic colorectal cancer (mCRC) was reported at ESMO 2006. Dose limiting toxicities (DLTs) were grade 3 stomatitis/pharyngitis, nausea, diarrhea, ileus and exanthema. The recommended doses (RDs) for this phase II portion were determined to be S-1 40-60 mg/body and LV 25 mg/body orally given twice daily on days 1 to 14 of a 28-day cycle. The PK profiles of S-1 plus LV were similar to those of S-1 monotherapy and UFT plus LV, respectively. The main purpose of this phase II portion is to evaluate the efficacy and safety of S-1 plus LV at RD level in pts with untreated mCRC. Methods: Pts were eligible as follows; unresectable mCRC with no prior chemotherapy or receiving adjuvant chemotherapy completed at least 6 months before, histologically proven adenocarcinoma, PS(ECOG) 0-2, age 20 to 75, measurable lesions, adequate organ function and written informed consent. The pts received 40-60 mg/body of S-1 plus 25 mg/body of LV twice daily as RD in this phase II portion. The primary endpoint was the objective response rates (RRs), and secondary endpoints were time to progression (TTP) and toxicities. Results: Between Sep 2004 and Jun 2006, 56 pts of 65 enrolled pts received the treatment at RD level. The objective RRs were 57% (37 of 65) for all pts and 57% (32 of 56) for pts at RD, extramurally. Disease control rates (DCRs) were 86% (56 of 65) for all pts and 86% (48 of 56) for pts at RD. Median TTP was 6.8 months for pts at RD. The median survival time is under investigation. During the 6 courses from starting the treatment, the most common grade 3/4 toxicities at RD were as follows: neutropenia, 13%; diarrhea, 27%; stomatitis, 20%; and anorexia 21%. Conclusions: A combination of S-1 plus oral LV is an effective, well tolerated, and convenient regimen in pts with untreated mCRC, without the addition of either oxaliplatin or irinotecan. This trial was supported by Taiho pharmaceutical co., Ltd., Tokyo, Japan.
Biological action of S-1 and Leucovorin A novel oral fluoropyrimidine derivative consists of 1M tegafur (FT; prodrug of 5-FU), 0.4M of gimeracil (CDHP) and 1M of potassium oxonate (Oxo) A oral leucovorin (LV) enhances anti-tumor activity of S-1
Background Study Rationale S-1 monotherapy showed promising activity (response rate (RR) of 37% as 1st line chemotherapy) against previously untreated metastatic colorectal cancer (mCRC) with conventional dosage (40-60 mg/body BID) and schedule (28 days of administration periods followed by 14 days rest) Better activity against mCRC is expected when leucovorin (LV) is orally administered with S-1 The efficacy and safety of S-1 plus oral LV have not been studied yet in clinical trials
Summary of Phase I portion DLTs were diarrhea, stomatitis/pharyngitis, nausea , ileus, and exanthema Level 2 (S-1 28 days administration) is the maximum tolerated dose (MTD) of this combination therapy Level 0 (S-1 14 days administration) is the recommended dose (RD), in terms of the continuity of planned 2 courses without any cessation or dose reduction S-1 plus oral LV may be promising treatment against untreated mCRC, achieving a high response rate of 66.7 % (95% confidence interval; 38.4~88.2 %) The PK parameters of S-1/LV, especially 5-FU and 5-MeTHF, were similar to those of S-1 alone and UFT/LV, respectively Administration periods of S-1/LV Dosage of S-1: 40-60 mg/body BID Dosage of LV: 25 mg/body BID administered orally together with S-1
Summary of Phase I portion(continue) PK parameter ** The PK parameters were recalculated using those from two previous studies1,2). The values of concentrations at the same sampling time with the present S-1/LV study were used in calculation, and the data from patients with gastrectomy were excluded from this analysis. 1) Hirata K. et al., Clin Cancer Res 5 2000-2005 (1999) 2) Shirao K. et al., J Clin Oncol 22 (17) 3466-3474 (2004)
Objectives Primary endpoint To assess the response rate of S-1/LV at the RD Secondary endpoints To evaluate the following at the RD the safety profile the efficacy about Time to progression (TTP) Time to treatment failure (TTF) Overall survival (OS)
Key Eligibility Criteria Histologically or pathologically confirmed colorectal adenocarcinoma Advanced, metastatic and unresectable cancer with measurable disease No prior chemotherapy for the metastatic disease. The adjuvant chemotherapy was allowed if chemotherapy had finished more than 180 days before the entry. Age 20 – 75 years Performance Status (ECOG scale) : 0-2 Adequate hematological, renal and liver function Life expectancy > 90 days Written informed consent
< 1.5 Treatment S-1: 40-60 mg/body BID Initial dosage Body surface area (m2) (tegafur equivalent) 40 mg BID < 1.25 50 mg BID 1.25 - < 1.5 - 60 mg BID LV: 25 mg/body BID administered orally together with S-1 S-1+LV p.o. BID 2 wks-on 2wks-off
Statistical Analysis RR of S-1 monotherapy was 16.7% - 39.5% Defined as minimum activity was 30% and target activity was 50% error was 0.05 and error was 0.2 We estimated 54 patients (pts) of full analysis set were required
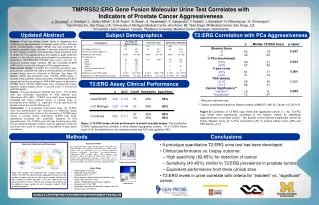
Results of phase I/II portion at the recommended dose Patients and Assessments Period From October 2005 to June 2006 Center 12 centers Patient 56 pts (6 pts – phase I portion) Response RECIST (extramurally) Safety NCI CTCAE v3.0
Treatment Courses Total courses during the 6 courses from starting the treatment
Efficacy Response Rate CI: Confidence Interval *: reviewed extramurally
Relative Dose Intensity (RDI) of S-1 During the 6 courses from starting the treatment RDI(%) is calculated by actual DI based on planed DI
Time to Progression (TTP) TTP; 203 days (6.8 Months) [ 95%CI; 164.0~241.0]
Time to Treatment Failure (TTF) TTF; 182 days (6.0 Months) [ 95%CI; 164.0~237.0]
Overall Survival (OS) MST: not reached Median follow-up time : 447 days
Common Toxicities During the 6 courses from starting the treatment CTCAE v3.0
Reason for treatment Discontinuation level 0 (RD): Four pts are ongoing
Summary Promising anti-cancer effect of S-1 with oral LV is shown in this study Major adverse reactions are gastrointestinal toxicities, without Gr4 severe toxicities There are no treatment-related death and the incidence of treatment discontinuation due to toxicity is only 3.8%
Conclusions A combination of S-1 plus oral LV is an effective, well tolerated, and convenient regimen in pts with untreated mCRC Further investigations of this combination chemotherapy with adding other active agents, such as oxaliplatin and bevacizumab, are warranted
References Sugimachi K, et al. Oncology. 1999;57:202-210 Ohtsu A, et al. Br J Cancer. 2000;83:141-145 Shirao K, et al. Cancer 2004; 100: 2355-2361 Hyodo I, et al. ESMO 2006. Abstract #349P