Download

1 / 89
890 likes | 1.11k Vues
Metabolic Complications of HIV Infection and Antiretroviral Therapy (ART) . Christopher Behrens, MD University of Washington. Metabolic Complications of HIV Infection and ART. Lactic Acidemia Lipodystrophy Dyslipidemia Insulin Resistance Cardiovascular Disease

E N D
Metabolic Complications of HIV Infection and Antiretroviral Therapy (ART) Christopher Behrens, MD University of Washington
Metabolic Complications of HIV Infection and ART • Lactic Acidemia • Lipodystrophy • Dyslipidemia • Insulin Resistance • Cardiovascular Disease • Bone Mineralization Disorders
Lactic Acidemia & Lactic AcidosisDefinitions • Lactic Acidemia: serum lactate level greater than 2.0 mmol/L in conjunction with a normal serum pH • Common in HIV-infected patients on ART • Varying degrees of severity • Often asymptomatic • Lactic Acidosis: serum lactate level greater than 2.0 mmol/L in conjunction with a serum pH less than 7.30 • Reflects most serious form of lactic acidemia • Rare but potentially fatal • Common signs & symptoms include lethargy, fatigue, weight loss, nausea, abdominal pain, and dyspnea • Concomitant hepatotoxicity common with hepatomegaly, hepatic steatosis, and even ascites and encephalopathy Schambelan M et al. JAIDS 2002;31:257-75
0 Classification of Lactic Acidemia *Symptoms and signs that suggest lactic acidemia consist of nausea, vomiting, abdominal pain, weight loss, fatigue, myalgias, abdominal distention, abdominal pain, dyspnea, and cardiac dysrhythmias. Source: HIV Web Study (www.hivwebstudy.org); Schambelan M et al. JAIDS 2002;31:257-75
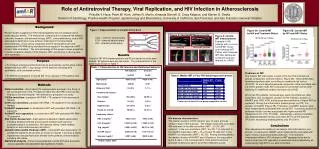
Proposed Pathophysiology of Lactic Acidemia NRTI-induced mitochondrial toxicity
0 NRTI-induced mitochondrial toxicity Proposed Pathogenesis CELL glucose MITOCHONDRION lactate pyruvate Acetyl CoA Krebs cycle Fatty Acids NADH FADH2 Oxidative phosphorylation ATP
0 NRTI-induced mitochondrial toxicity Proposed Pathogenesis CELL glucose MITOCHONDRION lactate pyruvate Acetyl CoA Krebs cycle Fatty Acids NADH FADH2 DNA pol γ mtDNA Oxidative phosphorylation ATP
0 NRTI-induced mitochondrial toxicity Proposed Pathogenesis CELL glucose MITOCHONDRION lactate pyruvate Acetyl CoA Krebs cycle Fatty Acids NADH FADH2 NRTIs DNA pol γ mtDNA Oxidative phosphorylation ATP
0 NRTI-induced mitochondrial toxicity Proposed Pathogenesis CELL glucose MITOCHONDRION lactate pyruvate Acetyl CoA Krebs cycle Fatty Acids NADH FADH2 NRTIs DNA pol γ mtDNA Oxidative phosphorylation ATP
0 NRTI-induced mitochondrial toxicity Proposed Pathogenesis CELL glucose MITOCHONDRION lactate pyruvate Acetyl CoA Krebs cycle Fatty Acids NADH FADH2 NRTIs DNA pol γ mtDNA Oxidative phosphorylation ATP
0 NRTI-induced mitochondrial toxicity Proposed Pathogenesis CELL glucose MITOCHONDRION lactate pyruvate Acetyl CoA Krebs cycle Fatty Acids NADH FADH2 NRTIs DNA pol γ mtDNA Oxidative phosphorylation ATP
0 NRTI-induced mitochondrial toxicity Proposed Pathogenesis CELL glucose MITOCHONDRION pyruvate lactate Acetyl CoA Krebs cycle Fatty Acids NADH FADH2 NRTIs DNA pol γ mtDNA Oxidative phosphorylation ATP
0 NRTI-induced mitochondrial toxicity Proposed Pathogenesis CELL glucose MITOCHONDRION lactate pyruvate Acetyl CoA Krebs cycle Fatty Acids NADH FADH2 NRTIs DNA pol γ mtDNA Oxidative phosphorylation ATP
0 NRTIs have different levels of mitochondrial toxicity • Rank: ddC/ddI/d4T > 3TC > ZDV > ABC for effects on mitochondrial DNA polymerase gamma1 • Tenofovir has low affinity for mitochondrial polymerase gamma2 • However, cases of severe hyperlactatemia have been reported in association with all NRTIs3 1. Kakuda TN. Clin Ther 2000 Jun;22(6):685-708 2. Johnson AA et al. J Biol Chem 2001 Nov 2;276(44):40847-57 3. Schambelan M et al. JAIDS 2002;31:257-75
0 Risk Factors for the Development of Lactic Acidemia in Persons Taking NRTIs *Most cases have involved stavudine**Especially with the use of stavudine plus didanosine Source: HIV Web Study (www.hivwebstudy.org)
0 Hyperlactatemia & Lactic AcidosisMeasuring Serum Lactate Levels • No vigorous exercise for 24 hours prior • Draw without tourniquet and fist clenching • Use pre-chilled gray top (fluoride-oxalate) tube • Place on ice and promptly send to lab; process within 4 hours • If increased, confirm with repeat measurement • Arterial pH measurement if frank acidosis suspected Schambelan M et al. JAIDS 2002;31:257-75.
0 Recommendations for the Management of Lactic Acidemia Source: HIV Web Study (www.hivwebstudy.org); Carr A. Clin Infect Dis 2003;36 (Suppl 2):S96-100.
Case • 44 year old male with C3 AIDS, well-controlled on ART regimen of d4T/3TC/efavirenz • Develops severe lactic acidosis and is admitted to the ICU • Recovers with discontinuation of ART and supportive care, but CD4 count now 290 cells/mm³, HIV viral load 66,000 copies/mL • What are your recommendations regarding antiretroviral therapy? • Do not resume ART – continue to monitor • Resume ART with efavirenz + lopinavir/ritonavir • Resume ART with TDF + 3TC + efavirenz • Resume prior ART regimen, supplemented with L-carnitine • I don’t know; just tell me the answer and get on with the talk
Resumption of Antiretroviral Therapy after Lactic Acidosis • NRTI-sparing regimen? • Promising early results from trials of efavirenz + lopinavir/ritonavir1 • Addition of mitochondrial-supporting compounds as prophylaxis against recurrent lactic acidosis? • Limited evidence of benefit in hastening recovery of patients with lactic acidosis, but efficacy in preventing the condition has not been established2-4 • Re-initiation of therapy using ‘mitochondria-sparing’ NRTIs (tenofovir, abacavir, 3TC, AZT)? • Reasonably safe in two studies5,6 1. Allavena C et al.JAIDS2005;39(3):300-306. 2. Fouty B et al. Lancet. 1998;352:291-2. 3. Lenzo NP et al. AIDS. 1997;11:1294-6. 4. Schramm C et al. Eur J Anaesthesiol. 1999;16:733-5. 5. Lonergan JT et al. AIDS. 2003;17:2495-9. 6. ESS40010 Study Team. JAIDS. 2004;36:935-42.
Case • 44 year old male with C3 AIDS, well-controlled on ART regimen of d4T/3TC/efavirenz • Develops severe lactic acidosis and is admitted to the ICU • Recovers with discontinuation of ART and supportive care, but CD4 count now 290 cells/mm³, HIV viral load 66,000 copies/mL • What are your recommendations regarding antiretroviral therapy? • Do not resume ART – continue to monitor • Resume ART with efavirenz + lopinavir/ritonavir • Resume ART with TDF + 3TC + efavirenz • Resume prior ART regimen, supplemented with L-carnitine • I don’t know; just tell me the answer and get on with the talk
Case 1 • 41 year old HIV-infected man on PI-based ART presents for routine follow-up • Complains of recent weight gain, especially in the abdomen • “It’s the protease paunch!”
Case 1 continued • PMH: • HIV infection x 5 years • Well-controlled on ART • CD4 nadir = 140 cells/mm³, most recent = 360 • No OIs, though radiology studies have suggested HIV encephalopathy • Hypertension • Medications: • d4T+ 3TC + lopinavir/ritonavir (Kaletra) x 2 years • Enalapril 10mg qd
Case 1 continued • PE: obese abdomen, otherwise unremarkable
What intervention would you recommend? • Ask his wife to padlock the fridge and get him a treadmill • Discontinue lopinavir/ritonavir, substitute an NNRTI such as efavirenz or nevirapine • Start metformin 500mg bid • Liposuction • None of the above have been demonstrated to improve HIV-associated visceral fat accumulation
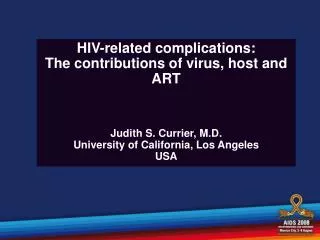
HIV/ART Toxicities: Lipodystrophy • Constellation of body habitus changes • Fat accumulation (lipohypertrophy): central (esp. visceral) fat, dorso-cervical fat pad (buffalo hump), breasts, lipomata, within muscle & liver • Fat wasting (lipoatrophy): face, extremities, buttocks, and trunk • Lack of clear case definition has hampered clinical research: wide variation in reported prevalence • Increasing evidence that lipoatrophy and lipohypertrophy are distinct entities, though can occur simultaneously • Hyperlipidemia and insulin resistance also variably present
Facial lipoatrophy Breast enlargement Central adiposity Peripheral lipoatrophy
FRAM Study: Defining Lipodystrophy Study Outline • Aim:compare randomly selected HIV-infected subjects and healthy controls to identify statistically significant differences and any linkages between lipodystrophic body changes • Three types of evaluation: • Self-report re: body habitus changes • Clinical evaluation of presence/degree of visible lipoatrophy • Body composition measures including whole-body MRI and DEXA scanning Grunfeld C. XIV International AIDS Conference, 2002, Abstract TuOr158.
FRAM: Defining Lipodystrophy • N = 565 men 33-45 years old • 412 HIV+ w/o OIs in past month • 153 HIV-negative controls from CARDIA study • Examined fat loss/deposition in peripheral sites (cheeks, face, arms, legs, buttocks) and central sites (waist, abdomen, neck, chest, upper back) • Peripheral and central lipoatrophy more common in HIV+ subjects • Central lipohypertrophy more common in HIV-negative subjects • Lack of concordance between lipoatrophy and lipohypertrophy Results for concordant self-report & exam % of patients p < 0.05 for all Gripshover B et al. 10th CROI, Boston, 2003, Abstract 732.
Lipodystrophy in Women: WIHS • Women’s Interagency HIV Study (WIHS): prospective, multi-site study of progression of HIV infection in women • 1,057 HIV-infected and HIV-uninfected women evaluated every 4 months over an 18-month period beginning in 1999 • Over 18 months, mean weight and total body fat increased slightly in HIV-negative women but remained stable in HIV-positive women • Incidence of peripheral and central lipoatrophy in HIV-positive women was double that of HIV-negative women • Incidence of central lipohypertrophy was similar in HIV-positive vs HIV-negative women Tien PC et al. 10th CROI, Boston, 2003. Abstract 736.
Lipohypertrophy Risk Factors Pathophysiology Interventions
0 Lipohypertrophy: Risk Factors • Duration of antiretroviral therapy • Use of protease inhibitors • Markers of disease severity • Age • Female gender Lichtenstein KA. JAIDS 2005;39:395-400.
Incidence & Size of Buffalo Humps N = 421 HIV(+) men vs 151 matched HIV(-) controls (FRAM cohort) p = NS p <0.001 % of patients Zolopa A et al. 10th CROI, Boston 2003, Abstract 734.
0 Lipohypertrophy: Pathophysiology
0 Lipohypertrophy: Treatment Options • Diet/exercise1-4 1. Jones SP et al. AIDS 2001 Oct 19;15(15):2049-51 2. Roubenoff R et al. Clin Infect Dis 2002 Feb 1;34(3):390-3 3. Roubenoff R et al. AIDS. 1999;13:1373-1375. 4. Thoni GJ et al. Diabetes Metab. 2002;28:397-404.
0 Lipohypertrophy: Treatment Options • Diet/exercise • Switching protease inhibitors out of ART regimen: inconsistent results Drechsler H, Powderly WG. Clin Infect Dis. 2002;35:1219-1230.
0 Lipohypertrophy: Treatment Options • Diet/exercise • Switching protease inhibitors out of ART regimen: inconsistent results • Diabetes agents? • Patients with lipodystrophy often demonstrate insulin resistance as well
0 Metformin Therapy for Lipohypertrophy? • N = 26 patients on ART with insulin resistance and fat redistribution • Randomized to metformin or placebo for 12 weeks Mean change in visceral abdominal fat, mm3 p = 0.08 Hadigan C et al. JAMA 2000;284:472-7.
0 Lipohypertrophy: Treatment Options • Diet/exercise • Switching protease inhibitors out of ART regimen: inconsistent results • Diabetes agents? • Plastic surgery?
0 Surgical Correction ofBuffalo Hump? • Liposuction or surgical excision a reasonable option, esp. if pain or functional limitations • Only small studies to date • Generally well-tolerated with favorable initial results • Conflicting data regarding recurrence: one study found a recurrence rate of just 5% (1/18 patients)1 while another study reported a recurrence rate of 50% (5/10 patients)2 1. Gervasoni C et al. 10th CROI, Boston, 2003. Abstract 723. 2. Piliero PJ et al. 10th CROI, Boston, 2003. Abstract 724.
0 What intervention would you recommend? • Ask his wife to padlock the fridge and get him a treadmill • Discontinue lopinavir/ritonavir, substitute an NNRTI such as efavirenz or nevirapine • Start metformin 500mg bid • Liposuction • None of the above have been demonstrated to improve HIV-associated visceral fat accumulation
0 Case 2: Lipoatrophy • 43 year old woman with history of PCP now doing well on ART: d4T/3TC/lopinavir/ ritonavir • She complains that her cheeks appear sunken and the veins in her arms and legs are more prominent
0 What intervention would you recommend for her condition? • Discontinue lopinavir/ritonavir, substitute atazanavir or an NNRTI • Discontinue d4T, substitute abacavir or tenofovir • Initiate rosiglitazone therapy • Plastic surgery: facial injections • None of these interventions is likely to help
0 Lipoatrophy: Risk Factors • Antiretroviral therapy • ART, esp. 2 NRTIs plus PI • d4T, esp. when used with ddI • Hierarchy: d4T/ddI/ddC > AZT > TDF/ABC/3TC • Prior AIDS diagnosis • Lower CD4 nadir • Lower body weight before ART • Caucasian race • Male gender • Older age Grinspoon S et al. N Engl J Med 2005;352:48-62. Podzamczer D et al. 11th CROI, 2004, Abstract 716. Lichtenstein KA et al. JAIDS 2003;32:48-56. Joly V et al. AIDS 2002;16:2447-2454. Dube M et al. 4th Int’l Workshop on Adverse Drug Reactions and Lipodystrophy in HIV, 2002, abstract 27. Shlay J et al. XV International AIDS Conference, 2004, Abstract ThOrB1360.
0 ? Etiology of Lipoatrophy: Evidence of Mitochondrial Toxicity in Adipocytes These are your mitochondria on ARVs These are your mitochondria J Acquir Immune Defic Syndr 2002 February 1;29(2):117-121
0 Lipoatrophy: Treatment Options • Switching d4T out of regimen: evidence for slow reversal of lipoatrophy
0 Abacavir substitution for patients with subcutaneous lipoatrophy (LA): MITOX • 111 patients with subjective LA on stable AZT- or d4T- containing ART randomized to substitute abacavir or continue current regimen1 • Limb fat mass measured by DEXA and by subjective physician assessment • Statistically significant increase in limb fat mass by DEXA at 104 weeks of follow-up2 • Similar findings from other studies3,4,5 Mean change in limb fat mass (intention-to-treat analysis) 4. JAIDS 2003;33:22-8. 5. JAIDS 2003;33:29-33. 1. JAMA 2002;288(2): 207-15. 2. AIDS 2004;18:1029-36. 3. CID 2004;38:263-270.