Download
1 / 75
750 likes | 784 Vues
Explore clinical cases, syndromes, and differential diagnoses of CNS infections with an emphasis on history and physical examination findings. Delve into acute versus chronic presentations, encephalitis versus meningitis distinctions, and important pathological considerations. Learn about anatomic relationships in the CNS.

E N D
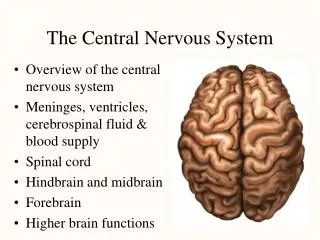
Infections of theCentral Nervous System Stephen M. Kralovic, MD, MPH Professor of Medicine Division of Infectious Diseases, University of Cincinnati Hospital Epidemiologist, Cincinnati VA Medical Center February 3, 2018
Case 1 • HISTORY • 43 year old previously healthy white male • Intermittent fevers • Headache • Speech difficulties • Left arm and leg weakness • This has all occurred over a 5-6 week period
Case 1 continued • PHYSICAL EXAM • Mildly obese • No neck stiffness ( no Brudzhinski’s sign) • Gingival retraction but no dental abscesses • No skin lesions • No lung or cardiac abnormalities • 4/5 left arm and forearm (distal and proximal) weakness with 4+/5 left thigh weakness • LABS • Peripheral CBC w/ WBC 16,200 (75% segs)
Case 1 continued • What do you think at this point? • Does the history give you any clues? • Do the physical exam findings suggest anything to you?
“Straw-Poll” VoteWhat entity is most likely present? • Brain abscess • Encephalitis • Meningitis-bacterial • Meningitis-viral (aseptic) • Spinal epidural abscess • Sepsis
Case 1 continued Patient felt to have a CNS tumor. Taken to surgery for radiation implants and purulence discovered.
Case 2 • HISTORY • 70 year old woman • Hypertension, hyperlipidemia, h/o MI 10 years ago • Presents for confusion and erratic behavior over the last couple of days • Low grade fever according to her spouse • Agitated—which is unusual for this woman
Case 2 continued • PHYSICAL EXAMINATION • T=101.2oF, HR=68, RR=16, BP=128/72 • Alert and oriented to self (A+Ox1) • Nothing else specific on physical examination • No focal neurological deficits • LABS • Peripheral CBC (WBC=7,500 w/61% segs)
Case 2 continued • Because of rapid onset of confusion in face of fever, lumbar puncture is performed • LP results: Cell count- WBC 7/mm3(lymphocytes) RBC 123/mm3 Glucose 53 mg/dl Protein 63 mg/dl CSF Pressure 138 mm H2O
“Straw-Poll” VoteWhat entity is most likely present? • Brain abscess • Encephalitis • Meningitis-bacterial • Meningitis-viral (aseptic) • Spinal epidural abscess • Sepsis
Case 2 continued *Sequential CTs of patient showing progressive destruction Viral culture of brain lesion grew Herpes Simplex Virus-I PCR of CSF was positive for HSV *from Chapter 8 “Herpes Simplex Virus” in Infections of the Central Nervous System-3rd Ed., 2004, ed. by Scheld, Whitley and Marra.
MRI • Herpes encephalitis • Predisposition for the temporal lobes • Coronal FLAIR magnetic resonance image from a patient with herpes simplex encephalitis. Note the area of increased signal in the right temporal lobe (left side of image) confined predominantly to the gray matter
Importance of History and Physical Examination • Give important clues as to whether infection is present or not • May give clues as the where or how infection was acquired • Trauma • Exposure • May give clues as to current location of infectious process • May give clues as to immune status of patient and risk for unusual (as well as usual) infections • Time of onset may give clues as to type of infection
Some things are pretty darned obvious from the history and physical exam…
Some cardinal manifestations SUGGESTING CNS infection Fever Headache Alteration of mental status Focal neurological signs • These are obtained from History and Physical Examination • Remember these are not specific for infection, but general for CNS pathology
Clinical Syndromes of CNS Infections • Acute vs. Chronic • Meningitis vs. Encephalitis vs. Myelitis • Symptoms • Space-occupying lesions • Other • Toxin mediated • Post-infectious syndromes • Prions (“slow viruses”) • Adapted from Chapter 1 in Infections of the Central Nervous System-3rd Ed., Lippincott, Williams, and Wilkins 2004, edited by Scheld, Whitley and Marra
Acute vs. Chronic • Acute--rapid or sudden onset • Usually hours to a couple of days • Clinical presentation may be quite dramatic or fulminate (e.g. “looks deathly ill”) • Chronic--slower more progressive onset • Usually several days to weeks to months or longer • Clinical presentation may not be as dramatic or fulminate • Subacute--somewhere between acute and chronic
Encephalitis vs. Meningitis • En•ceph•a•li•tis-- n. Pathology, Inflammation of the brain (a.k.a. “Brain fever”) • Men•in•gi•tis--n. Pathology, Inflammation of any or all of the meninges of the brain and the spinal cord, usually caused by a bacterial infection • The American Heritage Dictionary of the English Language: New College Edition, Houghton Mifflin Company, 1976
Know anatomic relationships • This is true for all neurological pathology • Remember CNS is enclosed both: • Anatomically • Physiologically (blood-brain barrier) • Immunologically • The immunological isolation may determine how infectious processes present
From Infections of the Central Nervous System, Ed by WM Scheld, RJ Whitley and DT Durack, 1991
From Infections of the Central Nervous System, Ed by WM Scheld, RJ Whitley and DT Durack, 1991
Keep in mind that what affects the brain can also affect the spinal cord Brain Spinal Cord Arachnoiditis Transverse myelitis Space-occupying lesions (e.g., spinal epidural abscess) Toxin-mediated syndromes Post-infectious syndromes • Meningitis • Encephalitis • Space-occupying lesions (e.g., brain abscess, subdural abscess) • Toxin-mediated syndromes • Post-infectious syndromes
Space occupying lesions • Clinical signs and symptoms will depend on anatomic location • Because of limited space in CNS focal findings on neurological examination may indicate the anatomic location of these lesions • e.g. • frontal lobe-personality, • motor cortex-upper motor neuron muscular weakness or focal seizure, • spinal canal-lower motor neuron weakness with sensory deficits • Brain abscess, spinal epidural abscess, neurocysticercosis
Toxin-mediated Syndromes • Infections occurring in locations other than CNS • Infecting organisms releases toxin into the host • Toxin has effect at site different than where infection is located • Examples: • Tetanus--stimulates nerves • Botulism--interrupts neural transmissions
Postinfectious Syndromes • Usually begins as another infection (many times sub-clinical or not considered to be noteworthy) • Infection may not be in CNS, but at distant site • Presumed to be immunologically-mediated • Examples: • Guillain-Barre • Post-infectious encephalomyelitis • ADEM (acute demyelinating encephalomyelitis)
Prions (“slow viruses”) • Considered to be unconventional infections • Truly chronic (years to decades in many cases) • Usually no fevers • High mortality • Examples: • Kuru, Creutzfeldt-Jakob disease (CJD), progressive multifocal leukoencephalitis (PML), “new-variant” Creutzfeldt-Jakob disease (nvCJD) (a.k.a. variant CJD)
CNS Syndromes From Durack, et al, Chapter 1 “Approach to the patient with central nervous system infection” in Infections of the Central Nervous System, Raven Press, 1997
How CSF may look in different inflammatory conditions From Rotbart, Chapter 3 “Viral meningitis and the aseptic meningitis syndrome” in Infections of the Central Nervous System, 1991 ed by Scheld, Whitley and Durack
Meningitis • This is the CNS infection entity that causes the most sensation • Especially acute, bacterial meningitis • When meninges inflamed, anything passing through them is at risk for involvement • Blood vessels feeding the cerebral cortex • Nerves exiting the brain (i.e. cranial nerves, especially those at the base of the brainstem)
Meningitis • Examples of purpura fulminans associated with severe Neisseria meningitidis infection from Chapter 23 “Acute Bacterial Meningitis” in Infections of the Central Nervous System-3rd Ed., 2004, ed. by Scheld, Whitley and Marra
TABLE 84-1 -- Differential Diagnosis of Acute Meningitis From Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases-7th Ed, Chap 84 Acute Meningitis
From Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases-7th Ed, Chap 84 Acute Meningitis
Meningitis • Common causes Bacterial, acute Streptococcus pneumoniae Neisseria meningitidis Group B Streptococcus (Streptococcus agalactiae) Listeria monocytogenes Haemophilus influenzae (hopefully vaccination against this organism will keep occurrence low) Others
Meningitis • Common causes continued Viral, acute Enteroviruses Viral, chronic Lymphocytic choriomeningitis virus Fungal, chronic Cryptococcus neoformans, Histoplasma capsulatum Mycobacterial, chronic Tuberculosis (Mycobacterium tuberculosis) Other Rickettsial, acute Rocky Mountain Spotted Fever Treponemal, both acute and chronic Syphilis, Lyme
Meningitis—U.S. Epidemiology 1 Schuchat, et al, N Engl J Med 1997;337:970-6.) Note the distribution in the age groups. Keep in mind that the numbers within these groups are not equal, so the rate of disease by age group is not proportional to the number of cases. Note also that Escherichia coli is not included in the analysis.
Management Meningitis--IDSA http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-Patient_Care/PDF_Library/Bacterial%20Meningitis(1).pdf
Adults http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-Patient_Care/PDF_Library/Bacterial%20Meningitis(1).pdf
Meningitis--Treatment • Empiric treatment based on rapid diagnostics (basic CSF picture and gram stain) and host characteristics • Knowing resistance patterns of common organisms in your geographic area is important (e.g. penicillin resistance in S. pneumoniae) • Getting a medication that crosses blood-brain barrier is important (easy when meninges are inflamed, but less so when not inflamed)
Adjuvant Therapy--Meningitis • Corticosteroids • Dexamethasone • Of value in children and adults with Streptococcus pneumoniae, Haemophilus influenzae b and Neisseria meningiditis. • First dose with or just before first dose of antibiotics to try to block TNF production
Empiric Presumptive Therapy http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-Patient_Care/PDF_Library/Bacterial%20Meningitis(1).pdf
Case 3 • 25 year old white male • 5-day history of headache • nausea, vomiting, photophobia and phonophobia, anorexia, fevers, chills and myalgias • HIV-infected (diagnosed ~5 years ago) • CD4 count 450+ cells/mm3, HIV viral = quantitation below level of detection • Diabetes x 7 years • Meds--efavirenz, zidovudine/lamivudine, rosiglitazone, esomeprazole, citalopram
Case 3 continued • PE • T=98.2oF, HR-79, RR-18, BP-122/77 • unremarkable otherwise • Labs • WBC 10,400 (normal differential), serum glucose 107 • CSF findings • No opening pressure recorded • 262 WBC (97% lymphocytes) • glucose = 62 • protein = 62
Case 3 continued • Viral culture of CSF no growth • Viral culture of rectal swab ordered--grew enterovirus • Gram stain without organisms seen • Bacterial culture no growth • CrAg = negative • HSV PCR = negative • ARBOviral serologies (acute) = non-diagnostic • West Nile PCR of both CSF and blood = negative
Aseptic meningitis (“viral meningitis”) • 85-95% of cases where causative agent identified are enterovirues • Enteroviruses • small ss +sense RNA viruses (picornaviruses) in a naked icosahedral capsid spread by the fecal-oral route and have a Summer-Fall seasonality in temperate climates • Include—polioviruses, coxsackieviruses, echoviruses, parechoviruses, and others simply designated enteroviruses • Treatment is supportive care
Encephalitis • CNS entity that causes a more global dysfunction (i.e. less likely to have focal neurological deficits, but can depending upon location) • Many times associated with viruses, but bacteria and other organisms may contribute to this • Herpes simplex encephalitis is not the most common; however, it causes serious morbidity and mortality. It is an important clinical entity in that it is one of the few viral encephalitides that can be effectively treated. Therefore, it is important to consider in a differential diagnosis.
The Burden of Encephalitis • Roughly 20,000+ cases annually • 50% etiology known (about half are infectious) • ~6% with a fatal outcome • Cost ~2 Billion dollars annually (2010 dollars) • Direct hospitalization only • No physician charges, no cost for subsequent rehabilitation • Seasonal peaks—late Summer/early Fall Vora, NM, et al, Neurology 2014;85(5):443-451
Treatment of Herpes Encephalitis • Supportive care • Antiviral agents with activity: • High-dose acyclovir or related agents Activated by viral thymidine kinase to become a competitive inhibitor of viral DNA polymerase by blocking deoxyguanosine uptake
Encephalitis—Epidemiology in US • ARBOviruses have some geographic propensity—St. Louis, California, Eastern Equine • West Nile encephalitis recently introduced into the US is causing some concern • Rabies predominantly from non-domestic animals—bats, skunks, coyotes, raccoons