Download
1 / 1
60 likes | 250 Vues
References:. Introduction:. Conclusion/Implications:. Patient Description:. Method:. A Case Report: Juvenile Myelomonocytic Leukemia Nina Muhammad, DO Department of Pediatrics, Advocate Hope Children’s Hospital. Diagnosis:. Significance of Case:

E N D
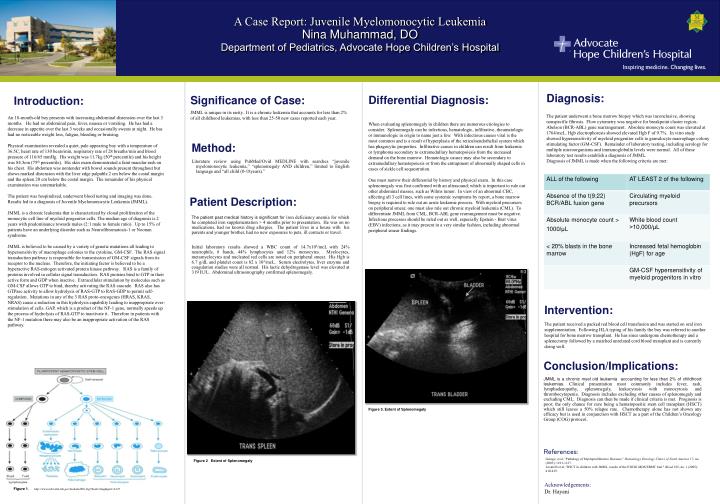
References: Introduction: Conclusion/Implications: Patient Description: Method: A Case Report: Juvenile Myelomonocytic Leukemia Nina Muhammad, DO Department of Pediatrics, Advocate Hope Children’s Hospital Diagnosis: Significance of Case: JMML is unique in its rarity. It is a chronic leukemia that accounts for less than 2% of all childhood leukemias, with less than 25-50 new cases reported each year. Differential Diagnosis: The patient underwent a bone marrow biopsy which was inconclusive, showing nonspecific fibrosis. Flow cytometry was negative for breakpoint cluster region-Abelson (BCR-ABL) gene rearrangement. Absolute monocyte count was elevated at 1764/mcL. Hgb electrophoresis showed elevated Hgb F of 9.7%. In vitro study showed hypersensitivity of myeloid progenitor cells to granulocyte macrophage colony stimulating factor (GM-CSF). Remainder of laboratory testing, including serology for multiple microorganisms and immunoglobulin levels were normal. All of these laboratory test results establish a diagnosis of JMML. Diagnosis of JMML is made when the following criteria are met: An 18-month-old boy presents with increasing abdominal distension over the last 3 months. He had no abdominal pain, fever, nausea or vomiting. He has had a decrease in appetite over the last 3 weeks and occasionally sweats at night. He has had no noticeable weight loss, fatigue, bleeding or bruising. Physical examination revealed a quiet, pale appearing boy with a temperature of 36.5C, heart rate of 130 beats/min, respiratory rate of 28 breaths/min and blood pressure of 116/65 mmHg. His weight was 11.7kg (50th percentile) and his height was 84.5cm (75th percentile). His skin exam demonstrated a faint macular rash on his chest. His abdomen was nontender with bowel sounds present throughout but shows marked distension with the liver edge palpable 2 cm below the costal margin and the spleen 20 cm below the costal margin. The remainder of his physical examination was unremarkable. The patient was hospitalized, underwent blood testing and imaging was done. Results led to a diagnosis of Juvenile Myelomonocytic Leukemia (JMML). JMML is a chronic leukemia that is characterized by clonal proliferation of the monocytic cell line of myeloid progenitor cells. The median age of diagnosis is 2 years with predominance towards males (2:1 male to female ratio). Up to 15% of patients have an underlying disorder such as Neurofibromatosis-1 or Noonan syndrome. JMML is believed to be caused by a variety of genetic mutations all leading to hypersensitivity of macrophage colonies to the cytokine, GM-CSF. The RAS signal transduction pathway is responsible for transmission of GM-CSF signals from its receptor to the nucleus. Therefore, the initiating factor is believed to be a hyperactive RAS-mitogen activated protein kinase pathway. RAS is a family of proteins involved in cellular signal transduction. RAS proteins bind to GTP in their active form and GDP when inactive. Extracellular stimulation by molecules such as GM-CSF allows GTP to bind, thereby activating the RAS cascade. RAS also has GTPase activity to allow hydrolysis of RAS-GTP to RAS-GDP to permit self-regulation. Mutations in any of the 3 RAS proto-oncogenes (HRAS, KRAS, NRAS) cause a reduction in this hydrolysis capability leading to inappropriate over-stimulation of cells. GAP, which is a product of the NF-1 gene, normally speeds up the process of hydrolysis of RAS-GTP to inactivate it. Therefore in patients with the NF-1 mutation there may also be an inappropriate activation of the RAS pathway. When evaluating splenomegaly in children there are numerous etiologies to consider. Splenomegaly can be infectious, hematologic, infiltrative, rheumatologic or immunologic in origin to name just a few. With infectious causes viral is the most common and is a result of hyperplasia of the reticuloendothelial system which has phagocytic properties. Infiltrative causes in children can result from leukemia or lymphoma secondary to extramedullary hematopoiesis from the increased demand on the bone marrow. Hematologic causes may also be secondary to extramedullary hematopoiesis or from the entrapment of abnormally shaped cells in cases of sickle cell sequestration. One must narrow their differential by history and physical exam. In this case splenomegaly was first confirmed with an ultrasound; which is important to rule out other abdominal masses, such as Wilms tumor. In view of an abnormal CBC, affecting all 3 cell lines, with some systemic symptoms by report, a bone marrow biopsy is required to rule out an acute leukemic process. With myeloid precursors on peripheral smear, one must also rule out chronic myeloid leukemia (CML). To differentiate JMML from CML, BCR-ABL gene rearrangement must be negative. Infectious processes should be ruled out as well, especially Epstein - Barr virus (EBV) infections, as it may present in a very similar fashion, including abnormal peripheral smear findings. • Literature review using PubMed/Ovid MEDLINE with searches “juvenile myelomonocytic leukemia,” “splenomegaly AND children,” limited to English language and “all child (0-18years).” The patient past medical history is significant for iron deficiency anemia for which he completed iron supplementation > 4 months prior to presentation. He was on no medications, had no known drug allergies. The patient lives in a house with his parents and younger brother, had no new exposures to pets, ill contacts or travel. Initial laboratory results showed a WBC count of 14.7x103/mcLwith 24% neutrophils, 8 bands, 44% lymphocytes and 12% monocytes. Myelocytes, metamyelocytes and nucleated red cells are noted on peripheral smear. His Hgb is 6.7 g/dL and platelet count is 82 x 103/mcL. Serum electrolytes, liver enzyme and coagulation studies were all normal. His lactic dehydrogenase level was elevated at 319 IU/L. Abdominal ultrasonography confirmed splenomegaly. Intervention: The patient received a packed red blood cell transfusion and was started on oral iron supplementation. Following HLA typing of his family the boy was referred to another hospital for bone marrow transplant. He has since undergone chemotherapy and a splenectomy followed by a matched unrelated cord blood transplant and is currently doing well. JMML is a chronic myel oid leukemia accounting for less than 2% of childhood leukemias. Clinical presentation most commonly includes fever, rash, lymphadenopathy, splenomegaly, leukocytosis with monocytosis and thrombocytopenia. Diagnosis includes excluding other causes of splenomegaly and excluding CML. Diagnosis can then be made if clinical criteria is met. Prognosis is poor; the only chance for cure being a hematopoeitic stem cell transplant (HSCT) which still leaves a 50% relapse rate. Chemotherapy alone has not shown any efficacy but is used in conjunction with HSCT as a part of the Children’s Oncology Group (COG) protocol. Figure 3. Extent of Splenomegaly George, et al, "Pathology of Myeloproliferative Diseases." Hematology Oncology Clinics of North America 17, no. (2003): 1101-1127. Locatelli et al, "HSCT in children with JMML, results of the EWOG-MDS/EBMT trial." Blood 105, no. 1 (2005): 410-419. Figure 2 Extent of Splenomegaly Acknowledgements: Dr. Hayani Figure 1. http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=hmg&part=A127