Peds PLACE
Community Based Research and Education (CoBRE) Core Facility. R. Whit Hall, MD, J. Hall-Barrow, EdD, and Edgar Garcia-Rill, PhD, Center for Translational Neuroscience and Dept. of Pediatrics University of Arkansas for Medical Sciences, Little Rock, AR. CAR Effects in the SubC.

Peds PLACE
E N D
Presentation Transcript
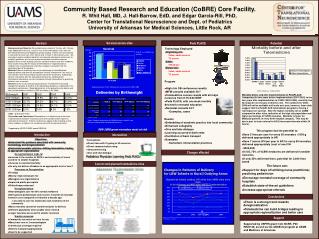
Community Based Research and Education (CoBRE) Core Facility. R. Whit Hall, MD, J. Hall-Barrow, EdD, and Edgar Garcia-Rill, PhD, Center for Translational Neuroscience and Dept. of Pediatrics University of Arkansas for Medical Sciences, Little Rock, AR CAR Effects in the SubC Survival across sites Peds PLACE Abstract Potential • Technology Employed • Originating site: • Video, audio camera • TV screen • Cable: • 750 kb/sec • Distant site: • Video, audio camera • TV screen Background and Objective We established a network of 15 sites, with 10 more to be added within the year, using T1 lines to link telemedicine units with real-time teleconferencing and diagnostic quality imaging. Fifteen units were placed in neonatal Intensive Care Units (NICU) and 10 more in other delivery sites. We carried out weekly combined obstetric and neonatal educational conferences to establish guidelines for the care of premature babies and other common pediatric illnesses with outlying clinicians caring for mothers and their newborns. Initial studies evaluated the impact of telemedicine on regionalization of newborn care, and of physician and other caregiver satisfaction with the educational part of the program. Methods Patterns of delivery were assessed through a linked Medicaid database before and after the telemedicine initiative to determine if the most at risk neonates were transferred to the perinatal center for delivery. Additionally, clinician satisfaction with the educational conference, combined with translational educational sessions, broadcast through telemedicine to practicing clinicians was assessed. Results Survey results from practicing clinicians revealed that they would change their practice to conform to the educational guidelines established in the educational conferences. Medicaid deliveries at the perinatal center before and after the telemedicine initiative in 2003 are shown in the Table. Program • High risk OB conferences weekly • MFM consults available 24/7 • Telemedicine census rounds with all major nurseries from 8:15-8:30 MWF • Peds PLACE, with one week monthly devoted to neonatal education • Neonatal consults 24/7 • Examples, cases Mortality before and after implementation of PedsPLACE. Comparing the two years before implementation (2001-2003) to the two years after implementation in 4/2003 (2003-2005), mortality has decreased in every type of delivery site. The numbers for 2006-2008 will not be available until early next year, however, these data suggest that the PedsPLACE telemedicine program is having a real impact on survival. Note the higher mortality rate at UAMS compared to other sites, indicative of the high risk population and higher percentage of VLBW neonates. Mortality is lower for Medicaid patients in every birth hospital category. This may be due in part to faster referral to ACH (increased referrals within 24 hours). This program has the potential to: • Save 5 lives per year for every 50 neonates <1000 g delivered appropriately in AR • Save 7 severe IVH per year in AR for every 50 neonates delivered appropriately (cost of one IVH ~$200,000) • In US, 75% of VLBW newborns are delivered in smaller nurseries • If only 25% delivered there, potential for 3,000 lives saved The future can: • Support for days off utilizing nurse practitioner, practicing pediatrician • Encourage neonatal coverage of community hospitals • Establish state-of-the-art guidelines • Increase appropriate referrals Table. *p<0.05 after 2002 Discussion and Conclusions Telemedicine is an effective way to translate evidence based medicine into clinical care when combined with a general educational conference. Patterns of deliveries appear to be changing so that those newborns at highest risk are being referred to the perinatal center. Supported by NCRR COBRE award RR20146. Results • Embedding of academic practice into local community • Enhanced collegiality • Give and take dialogue • Learning occurred at both ends • Facilitation of back transport • Examples • Surfactant, immunization practices Introduction Intervention • Objectives • Understand the problems associated with community neonatology and deregionalization • Understand possible solutions utilizing telemedicine leading to appropriate regionalization Deregionalization leads to: • Increase in the number of NICU’s and complexity of cases cared for in smaller hospitals • Increase in neonatal mortality • So why not deliver all babies in an appropriate level of care? Pressures to Deregionalize: • Prestige • Money: improved payer mix • Managed care organizations • Improved public perception • Philanthropy enhanced Deregionalization: • Neonatologists care for 60% normal newborns • BUT general pediatricians only receive 4 months of neonatal intensive care compared to 8 months a decade ago • Less able to care for moderately sick newborns in the community • Many neonates cannot be transferred prior to delivery • Different population when unable to be referred • Larger neonates do as well in smaller nurseries Smaller nurseries: • Community nurseries are here to stay • Many have one or 2 neonatologists • Continuous coverage required • Need to transport appropriately • Need to be supported • Telemedicine • Direct links with 10 going to 20 nurseries • Direct communication using videoconferencing • Give and take dialogue Pediatrics Physician Learning Peds PLACE Changes effected Current and planned telemedicine sites Conclusions • There is a strong trend towards deregionalization • Telemedicine can build bridges leading to appropriate regionalization and better care Support Supported by USPHS grant from NCRR, P20 RR20146, as well as the ANGELS program at UAMS and Medicare of Arkansas.