Download
1 / 14
300 likes | 1.09k Vues
THE ACUTE SCROTUM. Urology for Medical Students. THINGS YOU SHOULD KNOW AS A JUNIOR DOCTOR. TOPIC OUTLINE. CAUSES . ANATOMY OF TORSION. Types << Intravaginal twisted spermatic cord within tunica vaginalis Extravaginal >> twisted spermatic cord AND tunica vaginalis (in neonates).

E N D
THE ACUTE SCROTUM Urology for Medical Students
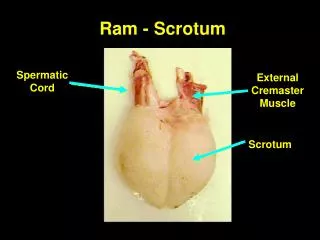
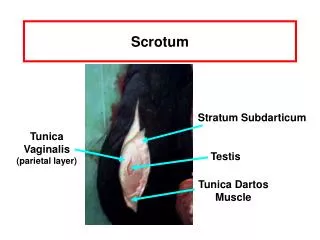
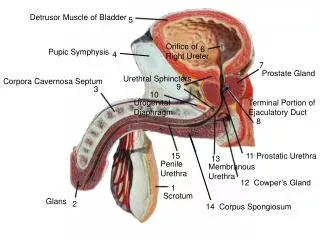
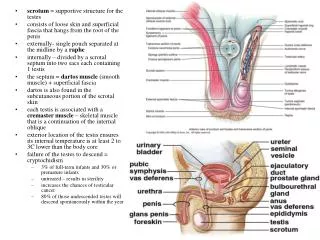
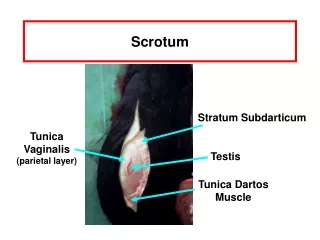
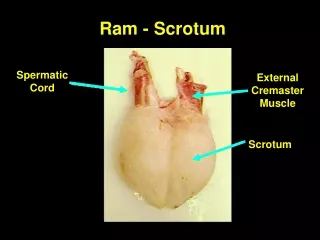
ANATOMY OF TORSION • Types • << Intravaginal • twisted spermatic cord within tunica vaginalis • Extravaginal >> • twisted spermatic cord AND tunica vaginalis (in neonates) • Structures • Testis • Appendix epididymis • Appendix testis
RISK FACTORS • Bell-Clapper deformity • Undescended testis Bell-Clapper Deformity (blue is tunica vaginalis)
TESTIS/EPIDYDIMIS INFECTION • Bacterial • UTI younger/older patients • usually gram negative bacteria • STD sexually active patients • Chlamydia trachomatis • Neisseria gonorrhoeae • Viral • Mumps
INVESTIGATIONS • Urine cultures • Urinary STD screen in sexually active • Doppler ultrasound • (Bloods + blood cultures) Doppler ultrasound Microscopy of E. coli
TREATMENT • Analgaesia & scrotal support • Urinary tract source (for 14 days) – empirical • Trimethoprim 300mg PO daily • OR cephalexin 500mg PO QID • OR augmentin 1tab PO BD • Sexually active young men – empirical • Ceftriaxone 500mg IV • AND Azithromycin 1g PO stat • AND Doxycycline 100mg PO BD (14 days) • If not improving exclude abscess • Ensure urine clear at end of antibiotics with U/A
FOURNIER’S GANGRENE • Necrotising fasciitis of genitalia & perineum • High mortality (30%) • Rapidly progressing • Risk factors – Diabetic, Immunocompromised, Alcoholic • Treatment • Rapid surgical debridement • Supportive care & broad spectrum antibiotics • Hypobaric oxygen
TRAUMA • Testicular Rupture • Requires prompt surgical repair • Can only be seen on US in 20% - go by clinical suspicion • Testicular Contusion/Intratesticular Haematoma • Hypoechoic or haetrogenous area on ultrasound • Usually explored because rupture cannot be excluded. • Then managed symptomatically: • Analgaesia • Scrotal support & elevation • Ensure resolution on follow-up ultrasound could be a testicular carcinoma!
REFERRED PAIN • Retrocaecal appendicitis • Urinary stones • Nerve root pain
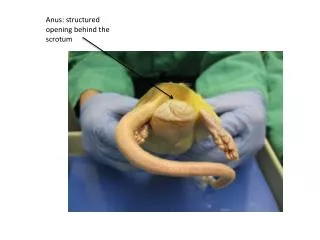
OTHER CAUSES • Varicocoele • Hydrocoele • Spermatocoele • Strangulated inguinal hernia • Heinrech-Scholein purpura (HSP) vasculitis • Testicular tumour (rapidly growing/necrotic)