The Importance of Self-Monitoring Blood Glucose in Achieving Good Glycemic Control
This guide emphasizes the critical role of Self-Monitoring Blood Glucose (SMBG) in managing diabetes and achieving optimal glycemic control. With over 25 million Americans diagnosed with diabetes, SMBG serves as a simple yet effective strategy to mitigate short- and long-term complications. Understanding SMBG's impact on HbA1c levels can significantly improve patient outcomes. This resource offers practical recommendations for healthcare providers and patients on integrating regular self-monitoring into diabetes care, thereby enhancing overall management strategies and quality of life.

The Importance of Self-Monitoring Blood Glucose in Achieving Good Glycemic Control
E N D
Presentation Transcript
Achieving Good Glycemic Control:The importance of Self Monitoring Blood Glucoseby:Nina Hibbard, CRNP StudentAuburn University/ Auburn Montgomery Joint Program
Aim Provide practical guidance on improving diabetes care through highlighting the need to: • Understanding of importance of SMBG • Improve overall control of diabetes patients • See the affects of SMBG on HA1C values
Definition and Description of the Problem Diabetes has been identified as one of the top 20 priority areas for national action according to the Institute of Medicine 25.8 million children and adults in the United States which is 8.3% of the population that have diabetes Self Monitoring Blood Glucose (SMBG) is a very simple way patients can control short and long term affects of diabetes complications
The numbers of diagnosed diabetes is growing stronger each year Diabetes: a global call to action 333 million 350 300 250 200 Global prevalence of diabetes (millions) 150 million 150 100 30 million 50 0 1985 2000 2025 Year http://www.idf.org/home/
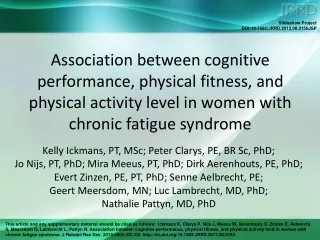
Diabetes is associated with serious complications Stroke 2- to 4-fold increase in cardiovascular mortality and stroke5 DiabeticRetinopathy Leading cause of blindness in adults1,2 CardiovascularDisease 8/10 individuals with diabetes die from CV events6 Diabetic Nephropathy DiabeticNeuropathy Leading cause of end-stage renal disease3,4 Leading cause ofnon-traumatic lower extremity amputations7,8 1UK Prospective Diabetes Study Group. Diabetes Res 1990; 13:1–11. 2Fong DS, et al.Diabetes Care 2003; 26 (Suppl. 1):S99–S102. 3The Hypertension in Diabetes Study Group. J Hypertens 1993; 11:309–317. 4Molitch ME, et al. Diabetes Care 2003; 26 (Suppl. 1):S94–S98. 5Kannel WB, et al. Am Heart J 1990; 120:672–676.6Gray RP & Yudkin JS. Cardiovascular disease in diabetes mellitus. In Textbook of Diabetes 2nd Edition, 1997. Blackwell Sciences. 7King’s Fund. Counting the cost. The real impact of non-insulin dependent diabetes. London: British Diabetic Association, 1996. 8Mayfield JA, et al. Diabetes Care 2003; 26 (Suppl. 1):S78–S79.
Individuals suffering ‘extreme problems’ in quality of life Diabetes General population 10.0 * 7.5 * Individuals reporting ‘extreme problems’ (%) * 5.0 2.5 * * 0 Anxiety/ depression Self-care Mobility Usual activities Pain/ discomfort *Significant versus general population Williams R, et al. The true costs of type 2 diabetes in the UK. Findings from T2ARDIS and CODE-2 UK, 2002. Department of Health. Health Survey for England 1996. London: HMSO, 1997.
Costs of diabetes are rising Indirect costs $132 140 Direct costs 120 $98 $92 100 80 Cost per year (US$ billion) 60 40 $20 20 0 19871 19922 19973 20024 Year Estimated US costs 1Huse DM, et al. JAMA 1989; 262:2708–2713. 2Javitt JC & Chiang Y-P. In Diabetes in America, 1995; 601–611. NIH Publication No. 95–1468. 3American Diabetes Association. Diabetes Care 1998; 21:296–309. 4American Diabetes Association. Diabetes Care 2003; 26:917–932.
Hospitalizations account for the majority of the costs of managing Diabetes Ambulatory care 18% Antidiabetic drugs 7% Other drugs 21% Hospitalizations 55% = €29 billion/year Jönsson B. Diabetologia 2002; 45 (Suppl.):S5–S12.
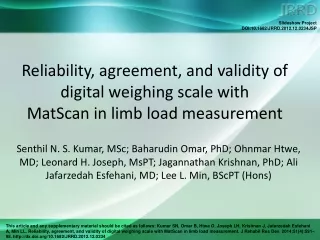
Lowering HbA1c reduces the risk of complications Deaths related to diabetes 21% HbA1c Microvascular complications 37% 1% Myocardial infarction 14% Stratton IM, et al. BMJ 2000; 321:405–412.
Two thirds of individuals do not achieve target HbA1c Saydah SH, et al. JAMA 2004; 291:335–342. Liebl A, et al.Diabetologia 2002; 45:S23–S28.
Barriers to achieving good glycemic control Lack of clarity over definition of good glycemic control Inadequate monitoring of glycemia Complexity of managing hyperglycemia relative to dyslipidemia and hypertension Insufficient involvement of physician and team
What is good glycemic control? The Global Partnership recommends: Aim for good glycemic control = HbA1c < 6.5%* < 6.5% *Or fasting/preprandial plasma glucose < 110 mg/dL (6.0 mmol/L) where assessment of HbA1c is not possible Del Prato S, et al. Int J Clin Pract 2005; 59:1345–1355.
Frequent monitoring of glycemia is important • Cornerstone of diabetes care • Ensures best possible glycemic control by: • assessing efficacy of therapy • guiding adjustments in diabetes care regimen, including diet, exercise and medications
Who should monitor glycemia? PatientSelf-monitoring of blood glucose + Healthcare professionalsRegular monitoring of HbA1c Diabetes care team Combined synergistic efforts of team are crucial to ensure effective monitoring of glycemic control
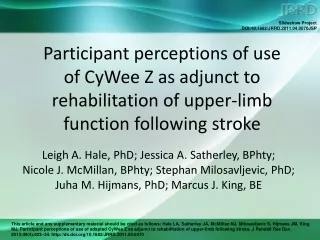
Not Monitored (37%) Regular SMBG Performers (21%) Irregular SMBG Performers (42%) Self-monitoring of blood glucose (SMBG) • Regular SMBG increases the proportion of individuals achieving their glycemic targets • Individuals should monitor postprandial glucose as part of their SMBG schedule • Regular discussion of results with diabetes care team is essential HbA1c 8.0 HbA1c > 8.0 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Blonde L, et al. Diabetes Care 2002; 25:245–246.
Physician input leads to better outcomes in type 2 diabetes 17% Individuals whom the physician was directly involved in proactive diabetes care had a substantially improved chance of survival Verlato G, et al. Diabetes Care 1996; 19:211–213.
Implementation PLAN: Present to two groups Group 1- Physician Group Group 2- Patient Group By presenting to two separate groups, the goal of the presentation is to make both more aware of the importance of SMBG and using this daily process as a useful tool in helping control diabetes in the short and long term.
Design • Physician Group- Current preceptor group of 4 doctors • *Powerpoint • *Evidence Based Research articles • *Demonstrate SMBG • *Enforce focus of management of patient more efficiently with this SMBG information • *Handouts provided for SMBG importance
Design • Patient Group- Group of diabetes patients identified at local retirement community. • *Verbal explanation and demonstration of SMBG provided • *Handouts provided for reinforcement • *Question and answer session
Delivery of Project Margaret Newman’s Theory of Health as Expand Consciousness • central thesis of this theory is that health is the expansion of consciousness • asserts that every person in every situation, no matter how disordered and hopeless it may seem, is part of the universal process of expanding consciousness” (Newman, 1992, p.60).
The Behavior and Skill of SMBG • Physician Group • Physicians will begin with a survey of how often they tell • their patients to check blood glucoses • SMBG demonstration • Insurance discussion
The Behavior and Skill of SMBG • Patient Group • Review of handouts • Discussion • Demonstration • Insurance discussion
Evaluation of Project Physician Group: Negative: *Do not have time to teach the patient *Too expensive for the patient * A1C test gives all information needed After discussion: Positive: *Realize the ease of local resources and meter companies to provide training *Understood insurance coverage of strips *Recognized useful in controlling medication regimen more efficiently
Evaluation of Project Patient Group: (31 Participants) Negative: * All patients did not have their own SMBG meter * Need not recognized. “My doctor keeps up with my blood sugar when I see him every three months.” * No understanding of insurance coverage Positive: *All patients end of session had a SMBG meter *Need recognized for daily monitoring and communicating to physician of blood sugar logs *Relieved to know of insurance coverage
Conclusion The educational project for SMBG awareness has been enjoyable and close to my heart. I truly have a passion for diabetes because it is very controllable with the right tools, support and education provided. This project is but the tip of the iceberg, but of great importance. I hope to continue to spread the news regarding SMBG and diabetes education for many years to come.
Acknowledgements Primary Care Internists of Montgomery, P.C. Dr. Raghu Mukkamala and partners 1722 Pine Street, Suite 309 Montgomery, Al 36106 Eastdale Estates Retirement Community 1500 Eastdale Circle Montgomery, Al, 36117