Chest Assessment
Chest Assessment. Read through the chart for past medical history and reasons for the present admission. Is the present admission for some other cause other than cardiopulmonary or is this a re-admission for a long standing chronic condition ? . Read the psychosocial history patient’s age

Chest Assessment
E N D
Presentation Transcript
Read through the chart for past medical history and reasons for the present admission.
Is the present admission for some other cause other than cardiopulmonary or is this a re-admission for a long standing chronic condition ?
Read the psychosocial history • patient’s age • marital status • supportive family (SW’s report) • will there be at-home care or will it involve some level of post-acute institutional care ?
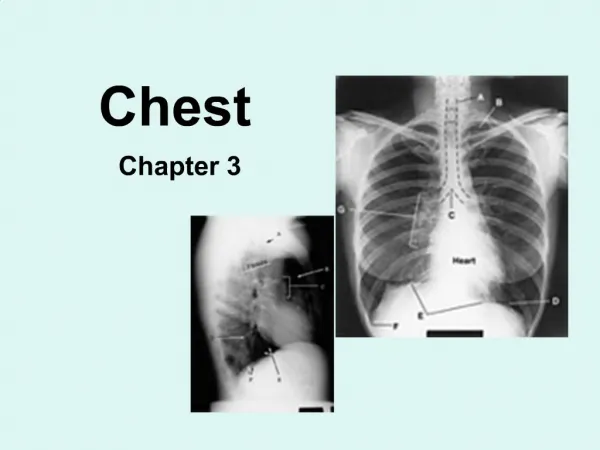
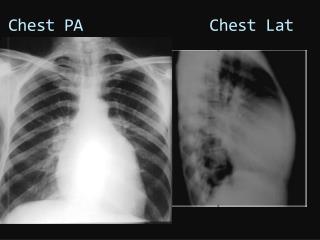
Look at the x-ray results : • Diffuse spider webbing ? • Egg-shell calcifications present ? • Is the cardiac image obscured ? • Are there spots on the lungs ? • Are fractures present ? • Fluid lines present ?
Read the pulmonary function test results • chronic obstructive lung disease • restrictive lung disease • occupational lung disease
Chronic Obstructive Disease • asthma • bronchitis • emphysema • bronchiectasis
Restrictive Lung Disease • sarcoidosis • tuberculosis • pneumonia • ARDS • IRDS • Valley Fever
Occupational Lung Disease • psiticosis • byssinosis - white lung • CWP - black lung • silicosis • asbestosis • pidgeon breeders disease
Read the blood gas report • Is the patient acidotic ? • Is the patient alkalotic ? • Has the patient metabolically compensated ?
Normal Blood Gas Values • pH = 7.35 - 7.45 • PO2 = 80 - 100 mm Hg • PCO2 = 36 - 44 mm Hg • HCO3 = 22 - 26 mEq/L
Read the bacteriology lab report for any infective organisms • gram positive bacteria • gram negative bacteria • yeast infections • HIV +
Gram Positive Bacteria : • staphylococcus - osteomyelitis • streptococcus - septicemia • clostridium - gangrene
Gram Negative Bacteria • salmonella - food poisoning • shigella - dysentery • klebsiella - pneumonia • pseudomonas - deep infections
Hemaglobin & Hematocrit okay ? • Hemaglobin : females - 13-14 g/dl males - 15 -16 g/dl • Hematocrit : females - 32 - 42 % males - 42 - 52 %
Briefly review the reports by the various services : • respiratory therapy • physician’s progress notes • social worker’s report • nurses notes
Patient Evaluation • Smoking History ? • S.O.B. & when did it start ? • Occupation ? Return to work ? • Is the patient ambulatory ?
Do they use portable oxygen ? • Are there positions of comfort ? • Talk Test
Physical Exam • Auscultate the lungs : • adventitious sounds • rales • rhonchi • pleural friction rub • stridor
Chest measurements - bilateral excursion - rib flare ? - ant/post movement of the chest ? • Breathing patterns • See-Saw breathing • diaphragmatic breathing • apical breathing
Double cough ? • Productive cough ? • Quantity of sputum • Color of sputum • Vocal fremitus ?
Patient’s color ? • CO2 narcosis - redness of skin • hypoxemia - cyanosis - blue cast • Mediate percussion • Surgical scars ?
Chest deformations ? • Pectus excavatum • Pectus carinatum • cavitations • barrel chest
Rate & depth of respiration • Dyspnic ? • Tachypnic ? • Nasal flaring ? • Accessory muscle use ?
Can the patient perform self-care ? • Can they roll in bed and come to sitting ? • Can they transfer into a chair ?
Can they walk in the room or out into the hall ? • Do they need supplemental oxygen at rest and during ADL’s or during exercise ?
Does the patient have pitting edema in the lower extremities ? • 1+, 2+, 3+, 4+ • CHF • renal failure • metastatic cancer
Patient Case Study # 1 • 82 y/o Caucasian female • Admitted for observation to EROU (23-hour stay): • falling • c/o of pain in chest and hip • PT consult : evaluation for level of medical care
Social History • Living alone in a rented apt. at Meridian Point - minor assisted living contract • Because of falling hx., Meridian Point would take her into their full assisted living units if she was admitted for 3 days at FMC
Family lives in Flagstaff, Az. • Family expressing reluctance about having her move in with them for companion care
Medical History • Fractured radius in Jan, 1999 • Fractured right femur in August, 1994 • Bilateral mastectomy - Cancer - 1980 • Pneumonia - 1980, 1990, 1996 • Negative for diabetes
Medical Findings • CT scan of thorax, pelvis WNL • CT scan of brain showed atrophy - WNL • X-Ray of chest showed some diffuse cloudiness in L > R - no masses
Physical Therapy Exam • ROM - WNL for all extremities • Strength - 4/5 for age • Gait - 125 ft without LOB w/ FWW • Transfers - SBA ---> min assist • Orientation - 3/3
Oximetry - SaO2 - 86% on 2 L/min as per nasal cannula • Blood Pressure - 156/88 • Heart Rate - 98 bpm
Breathing - diaphragmatic • Resp. rate - 18/min & shallow • Talk test - normal • No vocal fremitus present
Fever - 102° F • Subjective Symptoms : “I feel fine - I want to go home.”
Auscultation Of Thorax • mild crackles - left lingula, R middle lobe • medium crackles - bilateral anterior, lateral and posterior basilar BP segments • all other BP segments clear
Recommendations ? • Discharge to home with family for 24-hour companion care ? • Admission to hospital for 3 days and then to assisted living at Meridian Point ? • Back to Meridian Point and independent apartment living ?
Patient Case Study # 2 • 51 year old Native American female • Admitted to the hospital for : • inebriated pedestrian vs car • fractured right and left tibia and fibula in the distal 1/3 of both LE’s • fractured C3-C4 stable and non-displaced
multiple abrasions and lacerations • closed head injury • aspiration pneumonia
Physical Therapy Order : • Mobilize the patient - NWB on BLE’s • Functional activities
Social History • Lives with her daughter in Tolani Lake, Az. She herds cattle on a small ranch • Has a significant ETOH hx. • Has a significant psychiatric hx. • Has a significant spouse abuse hx. • Is now divorced
Medical History : • Repeated ETOH detox admissions to Aspen Hills - ‘92, ‘93, ‘95, ‘98 • Significant for appendicitis in ‘84 • Significant for hypertension • Significant for COPD (asthma) • Significant for hyperlipidemia • Significant for CAD - report of occasional angina on hard exertion
Physical Therapy Findings • Full ROM in all uneffected joints and extremities • Strength is WNL in BUE’s (5/5) BLE’s not tested
Bronchovesicular breath sounds in the bilateral posterior and lateral basilar bronchopulmonary segments of the bilateral lower lobes • A Monarch UE GXT was given - physical work capacity was Fair
BP at rest = 150/92 • BP at SLGXT = 212/100 • HR at rest = 78 BPM • HR at SLGXT = 168 BPM • Max METs obtained = 8.5