Download
1 / 1
10 likes | 287 Vues
15.62. 15.18. 16.00. 13.20. 14.00. 12.00. Adolescents (n=286). Adults (n=45). 10.00. 8.71. Score. 8.00. 6.00. 4.96. 4.51. 4.45. 4.42. 4.29. 3.84. 3.82. 4.00. 2.49. 1.15. 2.00. 0.84. 0.81. 0.56. 0.00. IMDS. DSS9. HSTS. AFSS. TSS. BCS*. ADHDS*. CDS*. Scale.

E N D
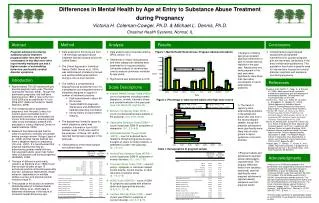
15.62 15.18 16.00 13.20 14.00 12.00 Adolescents (n=286) Adults (n=45) 10.00 8.71 Score 8.00 6.00 4.96 4.51 4.45 4.42 4.29 3.84 3.82 4.00 2.49 1.15 2.00 0.84 0.81 0.56 0.00 IMDS DSS9 HSTS AFSS TSS BCS* ADHDS* CDS* Scale Pregnant Adol. (n=328) Pregnant Adults (n=58) Never pregnant Adol. (n=3702) Never pregnant Adults (n=346) CDS* % with high level of problem ADHDS BCS 0.0% 10.0% 20.0% 30.0% 40.0% 50.0% 60.0% Differences in Mental Health by Age at Entry to Substance Abuse Treatment during Pregnancy Victoria H. Coleman-Cowger, Ph.D. & Michael L. Dennis, Ph.D. Chestnut Health Systems, Normal, IL Abstract Method Analysis Results Conclusions • Data analysis was conducted utilizing SPSS version 17.0. • Differences in intake characteristics and other categorical variables were examined by chi-square analysis. Univariate analysis of variance was used to analyze continuous variables by age group. • Significance was achieved at p<0.05. Pregnant adolescents entering substance abuse treatment programs differ from their adult counterparts in that they more often report weekly marijuana use and a higher number of externalizing behaviors--particularly conduct disorder symptoms. • Data analyzed in this study are from 118 individual substance abuse treatment facilities located across the United States. • The Global Appraisal of Individual Needs (GAIN; Dennis et al., 2003) was administered at intake by trained and certified GAIN administrators during a one-on-one interview. • The GAIN is a comprehensive biopsychosocial assessment tool. It is a progressive and integrated series of measures designed to support a number of treatment practices. • Staff-administered in about 60-90 minutes. • Yields DSM/ICD diagnostic impressions and ASAM/other treatment planning information. • Strong history of psychometric integrity. • The dataset was limited to cases for which pregnancy status was available. Information from 4,050 females (ages 12-53) was used for the analyses. Of these, 331 (8.2%) reported having been pregnant in the past year. • Characteristics of the entire sample are outlined below. Figure 1. Mental Health Scale Scores: Pregnant Adolescents/Adults • Comprehensive psychological assessment and targeted interventions for younger pregnant girls are warranted, particularly in the area of externalizing behaviors. This population has shown a specific need for interventions focused on conduct disorder symptoms and marijuana use during pregnancy. • Analysis of data by age group revealed significant difference in type of mental distress reported in the past year. Adolescents who were pregnant in the past year were significantly more likely than their adult counterparts to report externalizing problems. • The trend of reporting more externalizing problems in the adolescent group was also true in the never-pregnant sample, though the pregnant adolescents were significantly more likely than all other groups to report symptoms of conduct disorder. • Pregnant adults and adolescents reported similar demographic characteristics. The singular difference noted (from variables examined) was that significantly more pregnant adolescents reported weekly marijuana use than pregnant adults. Introduction References • Approximately 750,000 adolescent girls become pregnant each year (The Alan Guttmacher Institute, 2006). Though the adolescent pregnancy rate had been declining since 1990, it rose 3.4% from 2005-2006 and an additional 1% from 2006-2007 (National Center for Health Statistics, 2009). • The increasing rate of adolescent pregnancy over the past 2 years is a concern given that babies born to adolescent mothers are at elevated risk of poor birth outcomes, including higher rates of low birthweight, preterm birth, and death in infancy (National Center for Health Statistics, 2009). • Research has demonstrated that the odds of psychiatric morbidity are greater among younger women (Vesga-Lopez et al., 2008) and that mental distress can have a negative impact on pregnancy (Orr et al., 2007). It is hypothesized that pregnant adolescents may be experiencing greater mental distress than pregnant adults, given their higher rates of substance use during pregnancy (SAMHSA, 2008). • The type of distress is particularly relevant, as Bardone et al. (1996) found that conduct disorder at age 15 exclusively predicts antisocial personality disorder, substance dependence, illegal behavior, dependence on multiple welfare sources, and physical partner violence at age 21. • The purpose of this study is to examine Global Appraisal of Individual Needs (GAIN; Dennis et al., 2003) data to determine differences in the nature of comorbid mental distress by age. Scale Descriptions Bardone, A.M., Moffitt, T., Caspi, A., & Dickson, N. (1996). Adult mental health and social outcomes of adolescent girls with depression and conduct disorder. Development and Psychopathology, 8, 811-829. Dennis, M.L., Titus, J.C., White, M., Unsicker, J., & Hodgkins, D., Webber. R. (2003). Global Appraisal of Individual Needs: Trainer’s Training Manual and Resources. Bloomington, IL: Chestnut Health Systems. Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary data for 2007. National vital statistics reports, Web release; vol 57 no 12. Hyattsville, MD: National Center for Health Statistics. Released March 18, 2009. Martin JA, Hamilton BE, Sutton PD, Ventura SJ, et al. Births: Final data for 2006. National vital statistics reports; vol 57 no 7. Hyattsville, MD: National Center for Health Statistics. 2009. Substance Abuse and Mental Health Services Administration, Office of Applied Studies. (December 4, 2008). The NSDUH Report: Trends in Substance Use, Dependence or Abuse, and Treatment among Adolescents: 2002 to 2007. Rockville, MD. Vesga-Lopez, O., Blanco, C., Keyes, K., et al. (2008). Psychiatric disorders in pregnant and postpartum women in the United States. Arch Gen Psychiatry, 65, 805-815. • Internal Mental Distress Scale(IMDS) – count of symptoms including somatic, depression, anxiety, traumatic stress, and suicide/homicide in the past year. (Low 0-8; Mod 9-23; High 24-43) • Behavior Complexity Scale(BCS) – count of external behavioral problems in the past year. (0-5; 6-18; 19-23) • Depressive Symptom Scale (DSS9) – count of past year DSM-IV symptoms of depression. (0-1; 2-5; 6-9) • Homicidal/Suicidal Thought Scale (HSTS) – count of endorsed items related to killing/hurting someone else, thoughts of, plans for action towards, or attempted suicide in the past year. (0; 1-3; 4-5) • Anxiety/Fear Symptom Scale (AFSS) – count of past year DSM-IV symptoms of anxiety disorders. (0-1; 2-6; 7-12) • Traumatic Stress Scale (TSS) – count of past yr. symptoms or memories related to past trauma, current trauma, or other disorders of extreme stress. (0; 1-4; 5-13) • ADHD Scale (ADHDS) – count of DSM-IV symptoms associated with attention deficit and hyperactivity disorder. (0-5; 6-11; 12-18) • Conduct Disorder Scale (CDS) – count of past year DSM-IV symptoms of conduct disorder. (0-2; 3-7; 8-15) Figure 2. Percentage of Adolescents/Adults with High scale scores Table 1. Demographics of pregnant sample Acknowledgments Analysis of the GAIN data reported in this presentation was supported by Substance Abuse and Mental Health Services Administration's (SAMHSA's) Center for Substance Abuse Treatment (CSAT) under Contracts 207-98-7047, 277-00-6500, 270-03-00006, and 270-2007-00004C using data provided by grantees. The opinions expressed here belong to the author and are not official positions of the government. For more information, please contact Victoria H. Coleman-Cowger, Ph.D. * Chestnut Health Systems * 448 Wylie Drive * Normal, IL 61761 * 309-451-7797 * E-mail: vhcoleman@chestnut.org. The first author would like to acknowledge receipt of a 2009 NIDA Travel Award for this presentation at APA.