Download
1 / 38
380 likes | 637 Vues
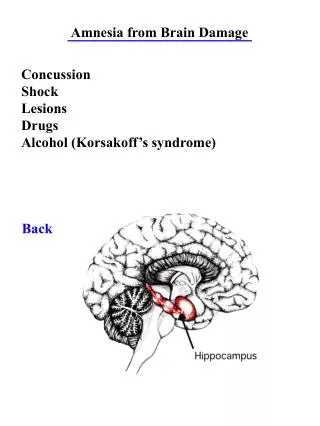
NEW INTERVENTIONS TO PREVENT PERINATAL BRAIN DAMAGE . Nigel Paneth MD MPH Michigan State University DC Children’s Hospital March 23, 2011. FOUR INTERVENTIONS SHOWN IN AT LEAST ONE APPROPRIATELY-POWERED RANDOMIZED TRIAL IN NEWBORNS TO SUCCESSFULLY REDUCE RISK OF CP IN SURVIVORS.

E N D
NEW INTERVENTIONS TO PREVENT PERINATAL BRAIN DAMAGE Nigel Paneth MD MPH Michigan State University DC Children’s Hospital March 23, 2011
FOUR INTERVENTIONS SHOWN IN AT LEAST ONE APPROPRIATELY-POWERED RANDOMIZED TRIAL IN NEWBORNS TO SUCCESSFULLY REDUCE RISK OF CP IN SURVIVORS. • IN TERM INFANTS • Therapeutic hypothermia • IN PRETERM INFANTS • Caffeine for apnea • MgSO4 administered in labor • Enriched infant formula
TWO INTERVENTIONS SOON TO BE TESTED • Infection/inflammation • Trial in the field • Thyroid hormone • Trial in preparation
INTERVENTIONS THAT HAVE NOT REDUCED CP IN APPROPRIATELY-POWERED TRIALS • Indomethacin • Repeat dose of betamethasone in labor • More liberal blood transfusion • Early hydrocortisone • Inhaled nitric oxide • Vitamin A • Etamsylate • Antenatal phenobarbital • HIFI Ventilation
THERAPEUTIC HYPOTHERMIA TO PREVENT CP RESULTING FROM PERINATAL ASPHYXIA
APGAR SCORES AND CEREBRAL PALSY IN INFANTS > 2,500 G Which column produced the most Children with CP?
THREE HYPOTHERMIA TRIALS WITH 18 MONTH OUTCOMES • Head cooling • Gluckman et al: Lancet 2005;365:663- 2005 • Whole body cooling by -4 °C • Shankaran et al: NEJM 2005;353:1574-83 • Whole body cooling by -3.5 °C • Azzopardi et al: NEJM 2009;361:1349-58
GLUCKMAN TRIAL • Mortality • OR = 0.81 (0.47 – 1.41) • Cerebral Palsy (described as severe neuromotor disability) • OR = 0.63 (0.25 – 1.17) • Death or disability • OR = 0.61 (0.34 – 1.09)
SHANKARAN TRIAL • Mortality • OR = 0.68 (0.44 – 1.05) • Disabling Cerebral Palsy • OR = 0.54 (0.38 – 1.22) • Death or moderate or severe disability • OR = 0.72 (0.54 – 0.95)
AZZOPARDI TRIAL • Mortality • OR = 0.81 (0.47 – 1.41) • Cerebral Palsy (described as severe neuromotor disability) • OR = 0.67 (0.47 – 0.96) • Death or severe neurodevelopmental disability • OR = 0.86 (0.68 – 1.07)
META-ANALYSIS(Edwards AD et al BMJ Feb 9 2010; 340: c397 • Three trials with 18 month outcomes • Death and severe disability risk ratio = 0.81 • 95% confidence interval 0.71 to 0.93 • Number needed to treat = 9 • Ten trials with mortality outcomes • Mortality risk ratio = 0.78 • 95% CI 0.66 to 0.93 • Number needed to treat = 14
“CAFFEINE FOR APNEA OF PREMATURITY” TRIAL - DESIGN • 2006 infants (BW 500 – 1250g) with apnea or at risk for apnea or needing ET removal. • 1,006 randomly assigned caffeine citrate, 20mg/kg loading dose + 5-10 mg/kg (as needed to control apnea) daily until 35 weeks of gestation. (mean GA 27.4 weeks) • 1,000 received placebo saline Schmidt et al: NEJM 2007;357:1893-1902
“CAFFEINE FOR APNEA OF PREMATURITY” TRIAL - RESULTS • Mortality • Treatment – 6.4% • Placebo - 6.5% • Adjusted OR = 0.99 (0.65 – 1.50) • Cerebral Palsy • Treatment – 4.4% • Placebo – 7.3% • Adjusted OR = 0.59 (0.39 – 0.89) • Death or disability • Treatment – 40.2% • Placebo - 46.2% • Adjusted OR = 0.79 (0.65 – 0.96)
OBSERVATIONAL STUDIES OF LABOR MgSO4 IN THE NINETIES • TWO CASE-CONTROL STUDIES • Schendel al: JAMA 1996;276:1805-10. • OR = 0.11, p< .05 • Nelson et al: Pediatrics. 1996;97:780-2 • OR = 0.15, p< .05 • ONE COHORT STUDY • Paneth N et al: Pediatrics 1997;97:723. OR = 0.63, NS
RANDOMIZED TRIALS OF LABOR MgSO4 IN THE CURRENT DECADE • Three randomized trials in premature labor • RR = 0.83 NS (< 30 weeks) Crowther 2003 [mortality OR = 0.83, NS] • RR = 0.63 NS (< 33 weeks) Marret 2008 [mortality OR = 0.79, NS] • RR = 0.55 p < .05 (24-31 weeks) Rouse 2008 [mortality OR = 1.12, NS] • One randomized trial in pre-eclampsia. • RR = 0.51 NS Magpie 2007 [mortality OR = 1.12, NS]
ENRICHED INFANT FORMULA Lucas et al: BMJ 1998; 317:1481-7
A PROPOSEDMAGNESIUM SULFATE PROTOCOL(Reeves SA et al AJOG march 2011;204:202e. 1-4 23-32 weeks, PTL or PROM and likely to deliver within 12 hours No contraindications (Mg sensitivity, already treated with Mg for PE, tocolysis) 6 grams IV over 20-30 mins, followed by 2 grams/hour until delivery for maximum of 12 hours
TRIAL OF ENRICHED INFANT FORMULA FOR BABIES < 1,850 g • Control arm – standard term baby formula • Intervention arm – formula enriched to provide • MACRONUTRIENTS • 33% more protein • 30% more fat • 17% more energy dense • MICRONUTRIENTS • Same amount: Mg, Mn, Vit A, choline • More electrolytes, Ca, Cu, Zn, I, Vitamins B1, B2, B6, B12, C, D, E, K, niacin, folate, panthothenic acid, taurine • Less iron, carnitine, inositol
RESULTS OF LUCAS TRIAL • Better weight gain and head circumference growth in neonatal period (p < .005) in enriched formula arm • IQ 3 points higher in intervention arm (NS), effect more pronounced in boys. • Cerebral Palsy • Intervention 1/68 = 1.5% • Term formula 8/67 = 12% • OR = 8.8 (1.1 – 72.4)
ORACLE 1 • 4,826 women with pre-labour rupture of the fetal membranes (pPROM) were randomly assigned to receive, four times a day for 10 days or until delivery, either: • 250 mg erythromycin (N = 1,197) • 325 mg co-amoxiclav, i.e. 250 mg amoxicillin + 125 mg clavulanic acid (N = 1,212) • Both antibiotics (N = 1,192) • placebo (N = 1,225) Kenyon et al: Lancet. 2001 Mar 31;357:979-88.
ORACLE 2 • 6,295 women in spontaneous preterm labour with intact membranes and without evidence of clinical infection were randomly assigned to receive, four times a day for 10 days or until delivery, either: • 250 mg erythromycin (N = 1,611) • 325 mg co-amoxiclav, i.e. 250 mg amoxicillin + 125 mg clavulanic acid (N = 1,550) • Both antibiotics (N = 1,565) • placebo (N = 1,569) Kenyon et al: Lancet. 2001 Mar 31;357:989-94.
ORACLE RESULTS AND FOLLOW-UP • In ORACLE 1 only, the erythromycin arm marginally reduced a composite neonatal outcome (neonatal death, chronic lung disease, or major cerebral abnormality on ultrasonography) by 20% 151 of 1190 [12.7%] vs 186 of 1225 [15.2%], p=0.08 • the ORACLE child study is following up the children in both trials at age 7 and assessing disability, including CP, by questionnaire
USING THYROID HORMONES TO PREVENT CP IN EXTREMELY PREMATURE INFANTS
THYROID HORMONE AND THE PREMATURE INFANT • When neonatal thyroid screening began in the 1970’s, premature infants frequently failed the screen because of low total T4. • Because TSH was not elevated, and T4 eventually normalized, prematures with low levels of T4 were not viewed with concern. • There is evidence however that “transient hypothyroxinemia of prematurity” (THOP) may not be benign.
EFFECTS OF NEONATAL THYROIDECTOMY IN THE RAT • Decreased levels of growth factors, brain protein and RNA synthesis • Less synaptogenesis • Reduction in enzymes necessary for nerve terminal development • Alterations in assembly of microtubule proteins • Delayed synthesis of myelin precursors • Diminished synthesis of enzymes required for myelin synthesis
THOP AND CEREBRAL PALSY BY GESTATIONAL AGE (T4 > 2.6 SD BELOW POPULATION MEAN)
STEPWISE ADJUSTMENTS IN ASSSESSING EFFFECTS OF THOP ON NEURODEVELOPMENT From Reuss et al NEJM 1996;334:821-7
THESE RESULTS LED TO THE THOP 1 TRIAL • Goal: Find dosage and administration method to maintain optimum thyroid hormone and TSH pattern • Conducted in NY, Madrid and Amsterdam • Six-arm study (N = 24 in each group) • Placebo, Iodine • Bolus T4: 4 μg vs 8 μg • Continuous T4: 4 μg vs 8 μg • Treatment from day 1 to age six weeks • Conclusion: Continuous 4 μg T4raises T4 acceptably with least suppression of TSH LaGamma E et al: Pediatrics. 2009 1242:e258-68
PHASE 3 TRIAL (THOP 2) 12-hospital Phase 3 trial applicatin has been submitted to NIH Intervention will be continuous T4: 4 μg for six weeks in infants < 28 weeks of gestation End point will be either CP at age two or percent with Bayley scores < 80 at age three. Sample size will be about 350 infants in each arm
CONCLUSIONS FROM NEWBORN TRIALS ABOUT CP REDUCTION Most neonatal treatments that are effective for neonatal outcomes do not seem to reduce CP. Very likely to be effective: Whole body cooling by 3-4 °C in perinatal asphyxia Probably effective: MgSO4 in preterm labor Possibly effective: Caffeine for apnea and fortified formula in prematures The jury is out on infection and thyroid hormone
NIH-FUNDED T-32 TRAINING PROGRAM IN PERINATAL EPIDEMIOLOGY AT MICHIGAN STATE UNIVERSITY
TRAINING IN PERINATAL EPIDEMIOLOGY AT MSU • Program funded by NICHD in May 2005 • The only T-32 training program in the nation focused solely on perinatal epidemiology • Support restricted by NIH rules to US citizens/green card holders • We have two post-doctoral positions per year • Support is for two years • Accepting applications for AY 2010-11 (earliest possible start date May 2011). • If interested, email cv, letter of interest to paneth@msu.edu
THANKS FOR LISTENINGI’M HAPPY TO TAKE QUESTIONS (This presentation is posted at http://www.epi.msu.edu/faculty/paneth.htm)