Download

1 / 38
420 likes | 1.27k Vues
Cri-du-chat syndrome. Imad Fadl-Elmula. History. In 1963, Lejeune et al., High-pitched. Microcephaly. Growth failure Abnormal face.. Mental retardation Facial abnormalities. Multiple congenital anomalies. Frequency. incidence 1 in 50,000 livebirths.

E N D
Cri-du-chat syndrome Imad Fadl-Elmula
History In 1963, Lejeune et al., • High-pitched. • Microcephaly. • Growth failure • Abnormal face.. • Mental retardation • Facial abnormalities. • Multiple congenital anomalies.
Frequency incidence 1 in 50,000 livebirths. 1.5 in 1000 among individual with mental retardation. Mortality/Morbidity 75% die within the first few months of life. 90% die before they are aged 1 year. Survival to adulthood is possible. Race No known racial predilection exists. Sex Male:Female ratio of 0.72.
Mechanism Most cases (80-85%) are due to sporadic de novo deletion of 5p. 30-60% of the cases involve terminal deletions with loss of 5p material. Approximately 10-15% of cases result from the unequal segregation of a parental balanced translocation where the 5p monosomy is often accompanied by a trisomic portion of the genome. Fewer than 10% of cases have other rare cytogenetic aberrations (eg, interstitial deletions, mosaicisms, rings and de novo translocations). The deleted chromosome 5 is paternal in origin in about 80% of the cases.
Cytogenetic analysis Normal Deleted
Phenotypes • The phenotypes and clinical features correlates with the size of loss region in 5p15.2 (cri-du-chat critical region).
Partial Monosomy:Cri-du-chat Syndrome (46,-5p) • Mental retardation, abnormal development of glottis and larynx • 1 / 50,000 live births
Characteristic cry • Newborns have the characteristic mewing cry, which is a high-pitched monochromatic cry that is considered. Pathognomonic. • This cry disappears by the time they are aged 2 years.
Clinical presentation 1. Speech. 2. Poor suck. 3. Motor delays. 4. Failure to thrive. 5. Severe cognitive. 6. Early ear infections. 7. Swallowing difficulties. 8. Early feeding problems.
Less frequently findings • Hypospadias, • Inguinal hernia. • Dislocated hips. • Cryptorchidism. • Gut malrotation. • Hydronephrosis. • Thymic dysplasia. • Cleft lip and palate. • Talipes equinovarus. • Renal ectopia or agenesis. • Preauricular tags and fistulas. • Clinodactyly of the fifth fingers. • Oligosyndactyly, and hyperextensible joints. • Rare renal malformations (horseshoe kidneys). • Syndactyly of the second and third fingers and toes.
Causes of death • Pneumonia. • Aspiration pneumonia. • Congenital heart defects. • Respiratory distress syndrome.
Behavioral history Behavioral profile includes • Aggression. • Clumsiness. • Hyperactivity. • Repetitive movements. • Hypersensitivity to sound. • Stereotypic and self-injurious behavior. • Features similar to those of autism
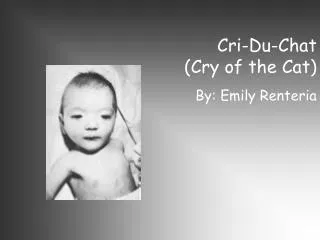
Image is of an infant with cri-du-chat syndrome. Note a round face with full cheeks, and apparently low-set ears
Facial laxity. • Dropped jaw. • Hypertonicity. • Small and narrow face. Patient with Cri-du-chat syndrome
Conventional cytogenetic • The size of the 5p deletion may vary from the entire short arm to only 5p15. • A small deletion of 5p may be missed by a conventional cytogenetic technique.
Chromosomal aberrations = 4 million base pairs = 0.13% of the genome New York Length of the haploid human DNA 4 million base would be equivalent to 8 km London London
Region - specific probe Fluorescence in situ hybridization • In patients with very small deletions. • The absence of a fluorescent signal from either the maternal or paternal chromosome 5p regions is indicative of monosomy for that chromosomal region.
Absence of a green signal indicates monosomy for that region (left, interphase cell; right, metaphase chromosome spread). Green is cri-du-chat locus signal. Orange color represents chromosome 5–specific signal
Late childhood and adolescence Findings include • Deep-set eyes. • Hypoplastic nasal bridge. • severe mental retardation. • Coarsening of facial features. • Prominent supraorbital ridges. • Severe malocclusion and scoliosis.
At puberty Female • Menstruate at the usual time. • The genital tract is normal in females. • Develop secondary sex characteristics. Males • Testes are often small. • Spermatogenesis is normal.
Consultations • Dentist. • Urologist. • Audiologist. • Neurologist. • Orthopedist. • Cardiologist. • Psychologist. • Ophthalmologist. • Clinical geneticist. • Developmental pediatrician. • Speech language pathologist. • Physical and occupational therapist.
Genetic counseling • Risk should be assessed based on the type of structural rearrangement and its pattern of segregation
Genetic counseling • Recurrence risk for affected female is 50%. • Recurrence risk for a de novo case is 1%. • If a parent is a balanced carrier of a structural rearrangement, the risk is substantially high. • Rare recurrences in chromosomally normal parents result of gonadal mosaicism for the 5p deletion in one of the parents.
Prenatal diagnosis Amniocentesis Routinely performed at 14-16 weeks’ gestation. Testing for chromosome disorders is 99.5% accurate. The missed are cases of mosaicism. The procedure is associated with a small risk of pregnancy loss (about 1 in 200 300).
Chorionic villus sampling (CVS) Timing Performed at 10-13 weeks’ gestation. Limitation and risk 1.Small chance of maternal cell contamination. 2. Risk of a fetal loss after the procedure 0.5-1%. 3. Accuracy less than Amniocentesis (mosaicism maternal cell contamination).
Percutaneous umbilical blood sampling (PUBS) Is of limited use, except in cases dated late in pregnancy.
Medical Legal Pitfalls Failure to: • Recognize characteristic symptoms and signs. • Refer to a geneticist for genetic counseling. • Request chromosome analysis of patients with the clinical phenotype of cri-du-chat. • Request chromosome analysis of parents to rule out familial translocation. • Offer prenatal diagnosis after the birth of an affected child.
Prognosis Activity Activities are limited because of profound mental retardation and physical handicaps. Patient Education Families are greatly affected. The main contributor to increased family stress is the child's maladaptive behavior. However, these families also receive social support from other families, friends, and concerned professionals.
Surgical Care • Correction of congenital heart defects may be indicated. • Orchiopexy for undescended testes. • Issues important to anesthetic plan: • Hypotonia. • Temperature maintenance. • Anatomical abnormalities of the airway. • Mental retardation Congenital heart disease.
Imaging Studies: • Skeletal radiography • Microcephaly, retromicrognathia • Cranial base malformations (reduced cranial base angle and malformed sella turcica and clivus) • Disproportionately short third, fourth, and fifth metacarpals and disproportionately long second, third, fourth, and fifth proximal phalanges (frequent)
Laryngeal appearance Floppy epiglottis. Small larynx. Asymmetric vocal cords. However, the cause of the characteristic cry cannot be entirely ascribed to the larynx. A developmental field connecting the brain and the affected clivus region of the cranial base with the laryngeal region from which the characteristic cry derives may exist. This area of the brain is probably deformed in patients with cri-du-chat syndrome. The characteristic cry usually disappears with time.
Magnetic resonance imaging • Atrophy of the brainstem, atrophic middle cerebellar peduncles and cerebellar white matter • Possible hypoplasia of cerebellar vermis with enlargement of the cisterna magna and fourth ventricle • Echocardiography - To rule out structural cardiac malformations • Other Tests: • Swallowing study for feeding difficulty • Comprehensive evaluation for receptive and expressive language: Most children have better receptive language than expressive language. • Developmental testing, referral to early intervention, and appropriate school placement
Childhood findings • Include severe mental retardation • Developmental delay • Microcephaly • Hypertonicity • Premature graying of the hair • Dropped-jaw, open-mouth expression secondary to facial laxity; short philtrum; malocclusion of the teeth; scoliosis; short third-fifth metacarpals; and chronic medical problems such as upper respiratory tract infections, otitis media, severe constipation, and hyperactivity.