Download
1 / 21
210 likes | 447 Vues
Epiretinal Membranes, CME and Macular Holes. Laura S. Gilmore, MD Grand Rounds November 14, 2003 Texas Tech University HSC Lubbock, TX. History. Chief Complaint: VA OD “fading away” x 6-8 months HPI: 81yo male referred for evaluation of chronic CME OD s/p CE 3 years ago

E N D
Epiretinal Membranes, CME and Macular Holes Laura S. Gilmore, MD Grand Rounds November 14, 2003 Texas Tech University HSC Lubbock, TX
History • Chief Complaint: VA OD “fading away” x 6-8 months • HPI: 81yo male referred for evaluation of chronic CME OD s/p CE 3 years ago • PMH: newly diagnosed DM with BS 120s-140s. HTN. Hypothyroidism. Arthritis. Hypercholesterolemia. • Ocular History: CE OD 99; KNOWN CME x 3 years • FH: diabetes, sister • SH: no alcohol. Quit smoking >30 years ago
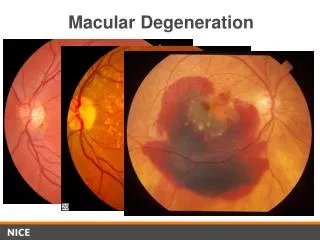
Physical Exam • VS: BP 115/79, P 74 • VA: OD 20/50 -1+2PH NI, OS 20/50 -1+1PH 20/40-2;VF FTFC OU x small central scotoma; AMSLER normal • IOP: OD 10, OS 14 • PCIOL OD, 3+ NSC OS • Anterior segment clear, without pupil distortion, PSC, synechiae, lens dislocation • DFE: OD-ERM; macular hole with flap of retinal tissue; multicystic CME; cryo scar supero-nasally; PVD with Weiss ring. OS-appears flat
Additional History • 1978: blunt trauma OD-champagne cork vs eye • Resultant RD, per patient • Treated in San Diego VA Hospital with cryotherapy, pneumatic retinopexy? • Still awaiting records from San Diego
Hypotheses • Senile macular hole • Blunt trauma caused retinal tear and/or detachment, and hole directly or indirectly • CME with ruptured cyst • Vitreofoveal traction syndrome 1st, then ERM • ERM 1st, leading to 1) tractional macular hole or 2) CME from ERM traction, then hole
Typical senile hole- not likely, since usually shows early hyperfluorescence Direct result of trauma in 1978? symptoms would have appeared within 6-12 months CME with ruptured cyst Not likely result of CE, or symptoms would have been evident within 6-8 months post-op. CE was over 3 years ago. Unlikely Choices
Most Likely Choice • RD repair/cryo, with resultant ERM 1st, leading to 1) tractional macular hole or 2) CME from ERM traction, then hole
Macular Dysfunction Caused by Epiretinal Membrane Contraction • Distortion • Intraretinal edema, CME • Degeneration of underlying retina
Classification by Distortion • Grade 0: Cellophane Maculopathy-translucent with no distortion of retina; cellophane light reflex • Grade 1: Crinkled Cellophane Maculopathy-irregular retinal folds and light reflex, radiating retinal folds; no to mild VA c/o, 20/40 at worst, +/-metamorphopsia, insidious onset • Grade 2: Macular Pucker-grayish membrane; marked retinal crinkling and puckering of macula; PVD in 90%; may see edema, retinal heme, CWS, SRD, leakage by FA; VA 20/200 or less, insidious to sudden onset, usually with metamorphopsia
ERM Following Retinal Tear/Detachment Repair • Grade 1 or 2 frequently seen s/p RT/RD repair • usually occurs 8-16 weeks post-op • VA in 20% of pts improves due to relaxation or partial peeling of ERM and resolution of intraretinal edema • Traction on macula can lead to hole or CME
Clinical Features of CME • Visual acuity is reduced according to severity and duration • Longstanding cases usually result in coalescence of fluid-filled microcysts into large cystic spaces • Lamellar holes form at fovea, causing irreversible damage to central vision • SLE shows loss of foveolar depression, thickening of retina, and multiple cysts in sensory retina
Signs of Macular Hole • Watzke-Allen-beam on foveola appears broken • round, red spot in the center of the macula, 1/3 to 2/3 DD, surrounded by a gray halo • lose foveolar depression; yellow spot in macula. • Small, yellow precipitates in hole subretinally • retinal cysts at the margin of the hole or a small operculum above the hole, anterior to the retina (stage 4) or both • May be caused by vitreous or epiretinal membrane traction on the macula, trauma, or cystoid macular edema
Fluorescein Angiography • CME-Dye accumulates in outer plexiform layer; Dye leaks into parafoveal region during the arteriovenous phase, coalesces into flower-petal pattern in late AV phase; hyperfluorescence from dye pooling in microcystic spaces persists through late phase • Macular/lamellar holes-EARLY hyperfluorescence • ERM-diffuse leakage of capillaries around FAZ; what we see
Summary • ERM following RD repair • tractional macular hole vs. CME from ERM traction, then hole
Proposed Treatment in this Case • Surgery at 20/50? F/U this week, 20/25 OD • No metamorphopsia, no Amsler symptoms • just small central scotoma • No; will follow. If VA decreases (at least 20/60) or pt has intolerable distortion, proceed with PPVx, membrane peeling
Gass, J. Donald M. Stereoscopic Atlas of Macular Diseases, Diagnosis and Treatment, Volume II, 4th Edition. 903-916, 938-954. Kanski, Jack J. Clinical Ophthalmology. 4th Edition. 424-425.