Download
1 / 66
660 likes | 722 Vues
Understand the etiology, pathogenesis, and classification of heart rhythm disorders, including arrhythmias, and their associated theories. Explore factors such as ANS activity changes, infection, toxins, mechanical influences, and ions imbalance affecting the heart's rhythm.

E N D
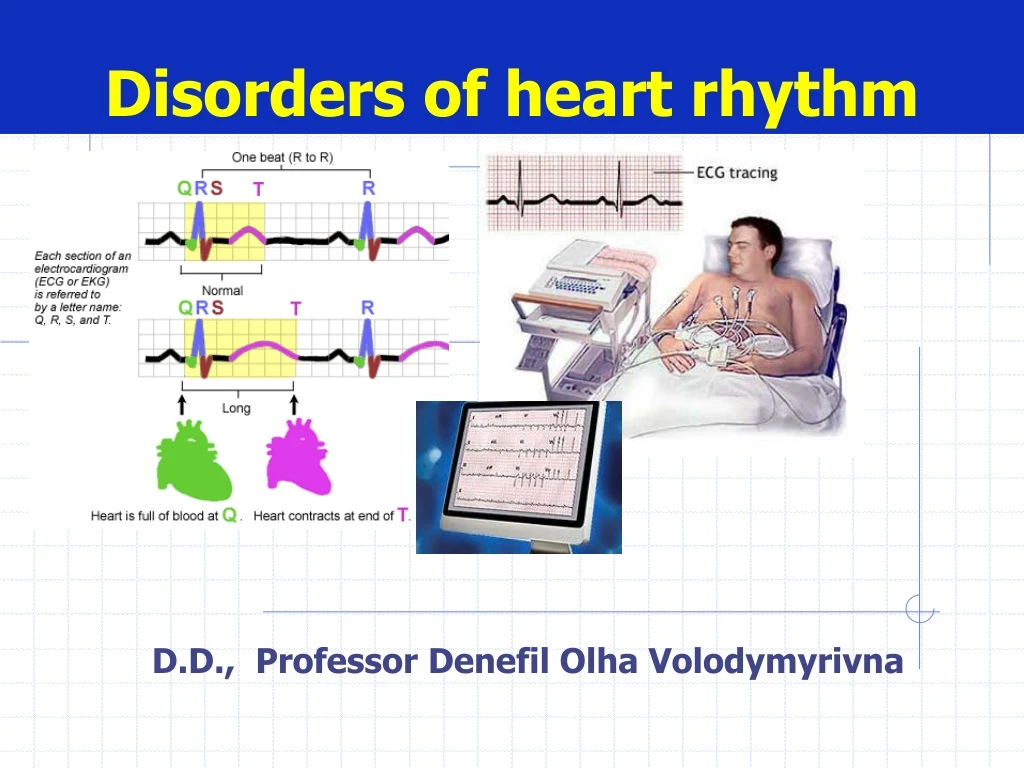
Disorders of heart rhythm D.D., Professor Denefil Olha Volodymyrivna
ETIOLOGY Functionalviolations and influences • ANS activity changes • Physical load • Body’st0change(fever; hyperthermia, hypothermia) • Hormone’s blood concentration changes • Intracranial pressure increase • Infection(flu, typhoid) • breathing(in children)
ETIOLOGY Organicfactors • inflammation of myocardium (infection, uninfection) • myocardial dystrophy (hypoxia, ischemia, amyloidosis) • myocardial necrosis
ETIOLOGY • Toxic influences - alcohol • medicines (beta-adrenoblockers) • catecholamine • glucocorticoids • bacterial toxins • phosphor organic substances
ETIOLOGY • Hormone balance violation • Hyperthyroidism • Hypothyroidism • suprarenal glandshyperfunction • suprarenal glands hypofunction
ETIOLOGY • Ions imbalance • changesofK, Na, Ca, Mg, Cl cardiomyocytes concentration (because long time using diuretics, uncontrolledusing mineral water) Organism more sensitive to К+deficit than to АТP one
ETIOLOGY • Mechanical influences • catheter using (for diagnosis and for treatment) • operation • chest trauma
PATHOGENESIS(pathological condition of the heart) • Injury of conductive system differentparts • No electrical homogenous of myocardium • No electricalfunctionalstableof myocardium(violation of MRP)
PATHOGENESIS(ARRHYTHMIAS THEORIES) Electricity of injury (No electrical homogenous of myocardium) Zone of injuryNormal tissue membrane is partlydepolarized membrane is completely depolarized (MRP = 0 mV or +20 mV) (MRP = -90 mV) potential difference appears between both these zones and ectopic driveractivates
PATHOGENESIS(ARRHYTHMIAS THEORIES) Ectopic rhythm driver activation (electricalfunctionalunstable myocardium ) Subthreshold oscillations : unstable MRP causeslow amplitude fluctuation, which can causeearly depolarization(hypoxia, K+ deficit, heart distention)
PATHOGENESIS(ARRHYTHMIAS THEORIES) Ectopic rhythm driver activation (electricalfunctionalunstable myocardium ) Overthreshold oscillations :appears at retardation or at breakingof repolarization (MAP cann’t be transformed in to MRP and new action potentialarrears and as a result - ectopic rhythm)
PATHOGENESIS(ARRHYTHMIAS THEORIES) “Re-entry” Nature:repeat or multiple impulses enter in some area of conductive system of the heart or in contractile myocardium Condition: • There are 2 conductive ways, which are separated functionally or structurally • There is block of impulses transmission thought the oneconductive way • Impulses transmission is possible only in reverse route
ARRHYTHMIAS CLASSIFICATION • Automatism violations • Conduction violations • Combined violations (automatism, conduction and excitability)
Automatism violation *Nomotopic(violation of impulsesformation in sinus node) 1. Sinus tachycardia 2. Sinus bradycardia 3. Sinus arrhythmia (respiratory) *Heterotopic rhythms(dominance of ectopic area activity) 1. Tardy ectopic rhythm (vicarious, passive) 2. Unparoxismal tachycardia 3. Migration of supraventricular rhythm driver
NomotopicAutomatism violationSinus tachycardia Reasons: physicalload, emotional stress, heart failure, myocardium ischemia or infarction, myocardium dystrophy ECG: sinus rhythm, HR90-180/min, R-R duration<0,60 c
NomotopicAutomatism violationSinus bradycardia Reasons: n. Vagus high activity (sportsmen, flu, typhoid),intracranial pressure increase (results from irritation of n.Vagus nucleas) ECG: sinus rhythm, HR59-40/min, R-R duration>1,0 с
NomotopicAutomatism violationSinus (respiratory) arrhythmia Reasons: breathing (in children), after viruses infections, neurocirculative dystonia ECG:sinus rhythm, difference between the shortest R-R and longestR-R >0,15 sec
Heterotopic rhythmsTardy (slowly) ectopic rhythm (vicarious, passive) Source:atrium, AV node, ventricle Meaning:protection of the heart at long time asystole (at SA node arrest) Kinds: -atrial -аtrial-ventricular • Ventricular (HR <40/min)
Heterotopic rhythmsaccelerated ectopic rhythm Unparoxismal tachycardia Source: atrium, AV node , ventricle ECG: -HR90-130/min - progressive beginning and finishing - regular ventriclerhythm
Heterotopic rhythmsMigration of supraventricular pacemaker Gradual removal of pacemaker from SA node to AV node ECG: P wave configurationviolation Change ofP-Q duration Arrhythmia
heart block Sinus atrial (or SA node arrest) - Intra Atrial - Atrial-ventricular -ventricular pre-excitation ventricular syndrome 1. WPW syndrome(Kent bundle) 2. CLC syndrome(James bundle) Conduction violations
Conduction violations Sinus atrial block (arrest) Violation of impulses transmission fromSA-node to atriums (most often - noncomplete) ECG:PQRST complex is absent compensatory pause is equal 2 (R-R) Some time 3-4PQRST complexes fall out and tardy ectopic rhythm (vicarious, passive) appears
Conduction violations Atrial block Violation of impulses transmission through the atrium conductive system ECG:Рduration>0,11 sec, Р -deformed (two waved)
Conduction violations АV-block Violation of impulses transmission through the AV node 1 degree 2 degree: Mobitz type I, Mobitz type II, type III(high degree AV block) 3 degree(complete AV block)
Conduction violations АV-block 1 degree ECG: PQ>0,2 sec
Conduction violations АV-block 2 degree *Mobitz type I (period of Venkebah) - Progressive increase ofPQ duration (Venkebah’s pariods)with after fall out QRST *Mobitz type II - PQare prolonged orNbut their length is constant QRSTfall out (periodicity is 2:1, some time 3:1, 4:1) * type III(high degree AV block) - QRSTfall out (periodicity is 2:1, 3:1, 4:1) bradycardia (tardy ectopic rhythm arrears) Symptoms: dizziness, unconsciousness
Conduction violations АV-block 3 degree (complete) * Absolute stop impulses conduction from atriums to ventricles * Independent excitation and contraction of the atriums and ventricles ECG: Рamount > QRS amount, P waves and QRS complexes appearindependently, some time Р are masked byQRS orT and that causes their deformation
Conduction violations АV block Stokes-Adams’s syndrome Reasons: - long timeasystole(more than 10-20 seс) (occurs at transition ofАV-block 2 degreetype IIIinto complete АV-block - long timeasystoleat АV-block3degree(complete) - long timeasystoleat ventricles fibrillation because АV-block3 degree Signs: unconsciousness, convulsions (because: decreased heart output and brain hypoxia) Prognosis:at every attack patient can die
Conduction violations ventricleblock • Violation of impulses conduction in ventricle conductivesystem Giss’sbundle branches block * blockof 1 branche * blockof 2 branches * blockof 3 branches * local intraventricleblock ECG:QRSdeformation
Conduction violations Pre-excitation syndrome WPW (Wolff-Parkinson-White) syndrome Reason: additional Kent’s bungle (impulses don’t transmit through the AV node but through Kent’s brunch) ECG: PQ<0,12 sec, QRS is deformed and wide because Δ-wave, ST и T arelocalized dyscordly, pre-excitation of the ventricles wave
Conduction violations Pre-excitation syndrome CLC (Clerk-Levy-Critesco) syndrome (syndrome of shortPQ) Reason: additional Jaims’s bungle(impulses came to ventricles earlier than through the AV node) ECG: PQ<0,12 sec, QRSunchanged
Conduction violations Pre-excitation syndrome Complications Pre-excitationofanyarea in ventricle Y Formation of electricalunstable myocardium Y “Re-entry”mechanism activation Y Ectopic driver appearens Y extrasistole paroxysmal tachycardia ventricle flutter (ventricular tachycardia)
Arrhythmias in the result of combined violations (automatism, conduction and excitability) • Extrasistole • Paroxysmal tachycardia • Atrium flutter • Atrium fibrillation • Ventricle flutter (ventricular tachycardia) • Ventricle fibrillation
Extrasistole extraordinary systole in the result of ectopic pacemaker activation Reason: * Membrane’shigh oscillative activity * “re-entry” mechanism Types, ECGsigns: - atrial(Р deformed) - atrial-ventricular(Р appears afterQRS) - ventricular(no Р before QRS, QRS deformation, complete compensatory pouse)
Extrasistole(atrial) ECGsigns: Р deformation
Extrasistole(from AV node) ECGsigns:Р appears afterQRS
Extrasistole(ventricular) ECGsigns:no Р before QRS, deformation ofQRS, complete compensatory pause
Paroxysmal tachycardia Attack of the heart contractions (140-250/min),which sudden onset and offsetat regular rhythm Mechanisms:- “re-entry”, ectopic driver activation Types, ECGsigns : - atrial (Р deformed) - atrial-ventricular (Р appears afterQRS) - ventricular(no Р before QRS, QRS is deformed and wide) Duration – from some seconds to some minutes
Atrium flutter rapid and regular atrial contructions with a rate from 240 to 450/min Mechanisms: re-entry, ectopic driver activation ECG: regular and rapid F-waves (sawtooth pattern), QRSunchanged