Download
1 / 1
20 likes | 206 Vues
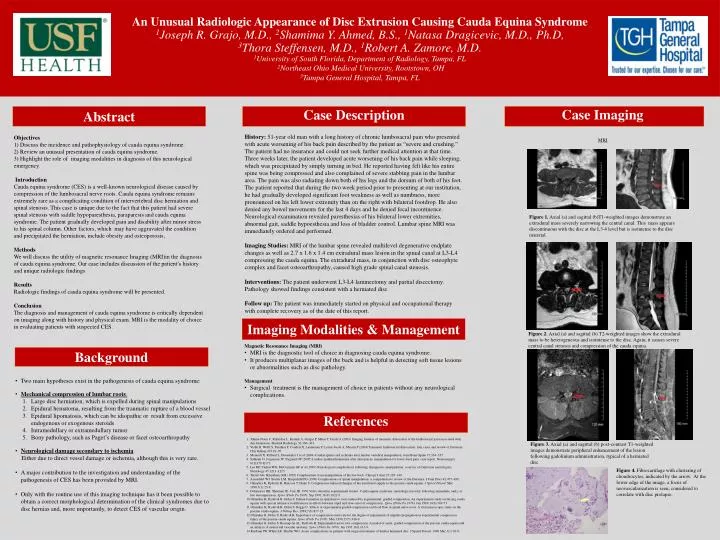
An Unusual Radiologic Appearance of Disc Extrusion Causing Cauda Equina Syndrome 1 Joseph R. Grajo, M.D., 2 Shamima Y. Ahmed, B.S., 1 Natasa Dragicevic , M.D., Ph.D , 3 Thora S teffensen , M.D ., 1 Robert A. Zamore , M.D.

E N D
An Unusual Radiologic Appearance of Disc Extrusion Causing CaudaEquina Syndrome • 1Joseph R. Grajo, M.D., 2Shamima Y. Ahmed, B.S., 1Natasa Dragicevic, M.D., Ph.D, • 3Thora Steffensen, M.D., 1Robert A. Zamore, M.D. • 1University of South Florida, Department of Radiology, Tampa, FL • 2Northeast Ohio Medical University, Rootstown, OH • 3Tampa General Hospital, Tampa, FL Case Imaging Abstract Case Description • History:51-year old man with a long history of chronic lumbosacral pain who presented with acute worsening of his back pain described by the patient as “severe and crushing.” The patient had no insurance and could not seek further medical attention at that time. Three weeks later, the patient developed acute worsening of his back pain while sleeping, which was precipitated by simply turning in bed.He reported having felt like his entire spine was being compressed and also complained of severe stabbing pain in the lumbar area. The pain was also radiating down both of his legs and the dorsum of both of his feet. • The patient reported that during the two week period prior to presenting at our institution, he had gradually developed significant foot weakness as well as numbness, more pronounced on his left lower extremity than on the right with bilateral footdrop. He also denied any bowel movements for the last 4 days and he denied fecal incontinence. • Neurological examination revealed paresthesias of his bilateral lower extremities, abnormal gait, saddle hypoesthesia and loss of bladder control. Lumbar spine MRI was immediately ordered and performed. • Imaging Studies: MRI of the lumbar spine revealed multilevel degenerative endplate changes as well as 2.7 x 1.6 x 1.4 cm extradural mass lesion in the spinal canal at L3-L4 compressing the caudaequina. The extradural mass, in conjunction with disc osteophyte complex and facet osteoarthropathy, caused high grade spinal canal stenosis. • Interventions: The patient underwent L3-L4 laminectomy and partial discectomy. Pathology showed findings consistent with a herniated disc • Follow up:The patient was immediately started on physical and occupational therapy with complete recovery as of the date of this report. Objectives 1) Discuss the incidence and pathophysiology of caudaequina syndrome. 2) Review an unusual presentation of caudaequina syndrome. 3) Highlight the role of imaging modalities in diagnosis of this neurological emergency. Introduction Caudaequina syndrome (CES) is a well-known neurological disease caused by compression of the lumbosacral nerve roots. Caudaequina syndrome remains extremely rare as a complicating condition of intervertebraldisc herniation and spinal stenosis. This case is unique due to the fact that this patient had severe spinal stenosis with saddle hypoparesthesia, paraparesis and caudaequinasyndrome. The patient gradually developed pain and disability after minor stress to his spinal column. Other factors, which may have aggravated the condition and precipitated the herniation, include obesity and osteoporosis, MethodsWe will discuss the utility of magnetic resonance Imaging (MRI)in the diagnosis of caudaequina syndrome. Our case includes discussion of the patient’s history and unique radiologic findings ResultsRadiologic findings of caudaequina syndrome will be presented. ConclusionThe diagnosis and management of caudaequina syndrome is critically dependent on imaging along with history and physical exam. MRI is the modality of choice in evaluating patients with suspected CES. MRI • Figure 1. Axial (a) and sagittal (b)T1-weighted images demonstrate an extraduralmass severely narrowing the central canal. This mass appears discontinuous with the disc at the L3-4 level but is isointense to the disc material. Imaging Modalities & Management • Magnetic Resonance Imaging (MRI) • MRI is the diagnostic tool of choice in diagnosing caudaequina syndrome. • It produces multiplanarimages of the back and is helpful in detecting soft tissue lesions or abnormalities such as disc pathology. • Management • Surgical treatment is the management of choice in patients without any neurological complications. Figure 2. Axial (a) and sagittal (b) T2-weighted images show the extraduralmass to be heterogeneous and isointense to the disc. Again, it causes severe central canal stenosis and compression of the caudaequina. Background • Two main hypotheses exist in the pathogenesis of caudaequina syndrome: • Mechanical compression of lumbar roots: • Large disc herniation, which is expelled during spinal manipulations • Epidural hematoma, resulting from the traumatic rupture of a blood vessel • Epidural lipomatosis, which can be idiopathic or result from excessive endogenous or exogenous steroids • Intramedullary or extramedullary tumor • Bony pathology, such as Paget’s disease or facet osteoarthropathy • Neurological damage secondary to ischemia: • Either due to direct vessel damage or ischemia, although this is very rare. • A major contribution to the investigation and understanding of the pathogenesis of CES has been provided by MRI. • Only with the routine use of this imaging technique has it been possible to obtain a correct morphological determination of the clinical syndromes due to disc hernias and, more importantly, to detect CES of vascular origin. References Tohme-Noun C, Rillardon L, Krainik A, Guigui P, Menu Y, Feydy A (2003) Imaging features of traumatic dislocation of the lumbosacral joint associated with disc herniation. Skeletal Radiology 32:360–363. Vialle R, Wolff S, Pauthier F, Coudert X, Laumonier F, Lortat-Jacob A, Massin P (2004) Traumatic lumbosacral dislocation: four cases and review of literature. ClinOrthop 419:91–97. Morandi X, Riffaud L, Houedakor J et al (2004) Caudal spinal cord ischemia after lumbar vertebral manipulation. Joint Bone Spine 71:334–337. Solheim O, Jorgensen JV, Nygaard OP (2007) Lumbar epidural hematoma after chiropractic manipulation for lower-back pain: case report. Neurosurgery 61:E170–E171. Lee KP, Carlini WG, McCormick GF et al (1995) Neurological complications following chiropractic manipulation: a survey of California neurologists. Neurology 45:1213–1215. Terrett AG, Kleynhans AM (1992) Complications from manipulation of the low back. Chiropr J Aust 27:129–140. Assendelft WJ, Bouter LM, Knipschild PG (1996) Complications of spinal manipulation: a comprehensive review of the literature. J FamPract 42:475–480. Olmarker K, Rydevik B, Hansson T, Holm S. Compression-induced changes of the nutritional supply to the porcine caudaequina. J Spinal Disord. Mar 1990;3(1):25-9. Delamarter RB, Sherman JE, Carr JB. 1991 Volvo Award in experimental studies. Caudaequina syndrome: neurologic recovery following immediate, early, or late decompression. Spine (Phila Pa 1976). Sep 1991;16(9):1022-9. Olmarker K, Rydevik B, Holm S. Edema formation in spinal nerve roots induced by experimental, graded compression. An experimental study on the pig caudaequina with special reference to differences in effects between rapid and slow onset of compression. Spine (Phila Pa 1976). Jun 1989;14(6):569-73. Olmarker K, Rydevik B, Holm S, Bagge U. Effects of experimental graded compression on blood flow in spinal nerve roots. A vital microscopic study on the porcine caudaequina. J Orthop Res. 1989;7(6):817-23. Olmarker K, Holm S, Rydevik B. Importance of compression onset rate for the degree of impairment of impulse propagation in experimental compression injury of the porcine caudaequina. Spine (Phila Pa 1976). May 1990;15(5):416-9. Olmarker K, Holm S, Rosenqvist AL, Rydevik B. Experimental nerve root compression. A model of acute, graded compression of the porcine caudaequina and an analysis of neural and vascular anatomy. Spine (Phila Pa 1976). Jan 1991;16(1):61-9. Kardaun JW, White LR, Shaffer WO. Acute complications in patients with surgical treatment of lumbar herniated disc. J Spinal Disord. 1990 Mar;3(1):30-8. Figure 3. Axial (a) and sagittal (b) post-contrast T1-weighted images demonstrate peripheral enhancement of the lesion following gadolinium administration, typical of a herniated disc Figure 4. Fibrocartilage with clustering of chondrocytes, indicated by the arrow. At the lower edge of the image, a focus of neovascularization is seen, considered to correlate with disc prolapse.