Download
1 / 28
280 likes | 388 Vues
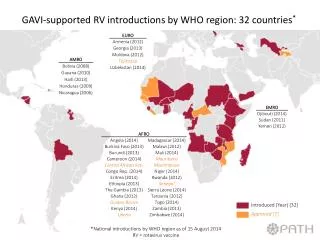
Update on HPV Susan Wang, WHO Tania Cernuschi, GAVI. IRC Briefing Geneva, 5 October 2012. Cervical Cancer Disease Burden and Programme Experience with HPV Vaccines. Cervical Cancer Incidence and Mortality Globally and By Region in 2008.

E N D
Update on HPVSusan Wang, WHOTania Cernuschi, GAVI IRC Briefing Geneva, 5 October 2012
Cervical Cancer Disease Burden and Programme Experience with HPV Vaccines
Cervical Cancer Incidence and Mortality Globally and By Region in 2008 • Overall, cervical cancer was responsible for 275,000 deaths worldwide in 2008, about 88% of which occurred in developing countries: 53,000 in Africa; 159,800 in Asia; and 31,700 in Latin America and the Caribbean. • High-risk regions are Eastern and Western Africa (Age-Standardized Rates greater then 30 per 100,000), Southern Africa (26.8 per 100,000), South-Central Asia (24.6 per 100,000), South America and Middle Africa (ASRs 23.9 and 23.0 per 100,000 respectively). • Cervical cancer remains the most common cancer in women in Eastern Africa and South-Central Asia.
Cervical Cancer Incidence Worldwide in 2008 Age-standardized incidence rates per 100,000 Available at http://globocan.iarc.fr/
Challenges with HPV vaccine introduction: common to any new vaccine introduction • Need to justify the vaccine addresses a public health priority and whether a non-vaccine intervention is available or better or cheaper than vaccine introduction • Need to assess costs of vaccine and delivery • Need to consider timeline and coordination with introduction of other new vaccines and other programme priorities • Need to create a new vaccine introduction plan and incorporate plan into country's comprehensive multiyear plan (cMYP) for the national immunization programme • Need to view vaccine as part of an integrated disease control and health promotion approach
Challenges unique to HPV vaccine introduction • Target population (9-13 year old girls): • Not previously served routinely by most immunization programs • In developing countries, similar health services not currently provided to this target population (services for nutrition, de-worming, malaria, HIV prevention, vision screening, etc. do not require health workers, injections, or cold chains) • Vaccine delivery • Needs 3 doses over the course of 6 months • Requires new routine delivery services and more social mobilization • Possible strategies: health center based, school-based, outreach in communities, campaign • Strategies need to be compatible with resources, affordable, sustainable, and achieve highest possible coverage
Challenges unique to HPV vaccine introduction:Costs of HPV vaccine delivery • Vaccine costs remain significant • Vaccine delivery costs (excluding vaccine costs) are significant for initial and recurring expenses. Currently available data based on WHO-PATH analysis suggest that for GAVI-eligible countries: • Start-up costs per girl for vaccine delivery are ~$3 • Operational costs for delivering 3 doses per eligible girl is ~$4.20 • During introduction year, total start-up and operational costs for delivering 3 doses per eligible girl is ~$7.20 (excludes vaccine cost)
Opportunitiesunique to HPV vaccine introduction • New stakeholders and partners • Not the traditional child health partners • Immunization, reproductive health, adolescent health, school health, cancer control, HIV prevention, women’s health • New energy and new advocacy • Interdisciplinary coordination needed
Lessons learned from national HPV vaccine introductions • When implementing HPV vaccine, every country has an array of problems to solve • Size of target population and location of target population (e.g., ideal grade to target) are often revised after the 1st and even the 2nd year of HPV vaccine use; delivery strategies may also need modification • Investments in IEC (information, education, and communication) are critical for HPV vaccine
Lessons learned from national HPV vaccine introductions: Schools • Where schools are used for vaccine delivery, • It is necessary to have • good coordination between Ministry of Education and Ministry of Health • engagement and education of local school staff • both high enrolment and high attendance of girls (for success, affordability) • It is helpful to make use of any existing infrastructure, such as school health coordinators or school immunization teams • In the absence of existing infrastructure or ongoing additional funding support, logistics and cost of using schools for delivery are not always sustainable • But to vaccinate girls who are least likely to access cervical cancer screening later in life, a country can not rely solely on school-based delivery
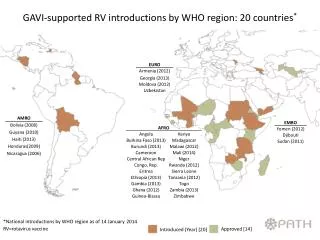
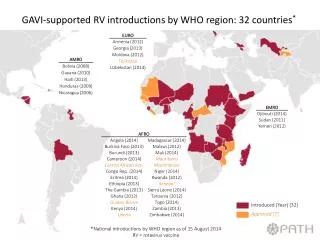
Why GAVI opened a funding window :Status of vaccine introduction worldwide Status as of July 2011 National HPV Programs GAVI eligible countries Source: Courtesy of Progress in Cervical Cancer Prevention: The CCA Report Card, August 2011
GAVI eligible countries and experience with HPV vaccine with existing or past experience with HPV vaccine no past experience with HPV vaccine Source: Courtesy of PATH – preliminary assessment of country readiness
Two Pathways for HPV vaccine introduction Country applications Country applications Natnl Intro (Pathway 1) Demo Program (Pathway 2) Demonstratedability needed Not approved Not approved Approved Approved Scale-up “Go/No-Go”? “Go” National Intro “No Go” Not Ready Applications from another pathway
Application National Introduction Requirements • Demonstrate at least 70% DTP3 coverage • Have demonstrated ability to deliver a complete series of vaccines • to at least 50% of the target vaccination cohort • in an average size district • using a similar strategy • Provide report on costing analysis of the proposed delivery strategy • Clarify plans for communication and social mobilization • National roadmap/strategy for a comprehensive approach to cervical cancer prevention and control, if possible
National Introduction – Main Features • Identify a single year of age or a single school grade cohort within the target population of 9-13 year old girls recommended by WHO • Identify one primary delivery strategy (e.g. school based, health facility based, outreach, mixed, or other) • 75% enrollment of the eligible population enrolled in school if school based delivery • If grade base strategy, the majority of girls must be between the ages of 9-13 years with no more than 20% of the girls aged 14 years or above.
Application and review process 2012 • Application window opened - June 2012 • Application submission deadline – 31 August 2012 • IRC review of applications – October 2012 • GAVI EC approval of applications – Early 2013 2 applications received: Rwanda and Uganda for support starting 2014
HPV Demonstration Programme: Objectives • Primary objective - Learn by doing: • Assessing potential HPV vaccine delivery strategies for coverage, feasibility, acceptability, and cost • Adapting and/or developing necessary tools • Secondary objectives: • Exploring the feasibility of integrating selected adolescent health interventions with the delivery of HPV vaccine • Encouraging integration of HPV vaccination in a national cervical cancer prevention and control strategy
HPV Demonstration Programme: Main Features • 2-years programme • Maximum size: 20,000 girls per year • Main activities: • Vaccination with selected strategy and evaluation of coverage, acceptability, feasibility, and cost of delivery • Assessment of the feasibility of integrating adolescent health or sexual and reproductive interventions with the delivery of HPV vaccine. If possible, testing of joint delivery • Develop or strengthen a comprehensive cervical cancer prevention and control strategy • A multi-stakeholder technical advisory group required to guide planning and implementation • No co-financing requirements • Programmatic grant provided
Application Process for HPV Demo -2012 • Application window opened - August 2012 • Application submission deadline - 31 October 2012 • IRC review of applications - Week of 19 November • GAVI CEO approval of applications - End December 2012 In future, timing of HPV demo windows to coincide with NVS support windows
To be updated: Number of National Introductions & Demonstration Projects • 40 GAVI supported introductions by 2020 • Up to 27 countries are forecasted to run demonstration projects with GAVI support by 2015; up to 40 by 2020 • GAVI supported demand to peak at 46m in 2026 • Over 32m girls projected to be immunized with HPV vaccines by 2020 with GAVI support
HPV Development Pipeline Source: AVI SVS
HPV demand from GAVI-eligible countries - Volume 70% reach of out of school girls