Download
1 / 31
310 likes | 327 Vues
Discover the unique characteristics and impact of Orthomyxoviruses, particularly Influenza or 'Flu.' Understand their structure, antigenic classification, variation, and transmission, as well as the pathogenesis and complications caused by these viruses.

E N D
ORTHOMYXOVIRUSES • Affinity for mucins (mucus) • Adsorb to mucoprotein receptors on RBC’s • Myxovirus – Ortho & Paramyxoviruses • Genus Influenza – Type A,B &C • Species of Type A- • H1N1(A1human, Hsw N1) • H2N2 (A2) • H3N2 (A3, A Hong Kong)
‘FLU’ • True influenza • influenza virus A or influenza virus B (or influenza virus C infections - much milder) • Febrile respiratory disease with systemic symptoms caused by a variety of other organisms often inaccurately called ‘flu’
Influenza - the Disease • Acute respiratory infection (ARI) with abrupt disease onset • Clinically it cannot be distinguished from other ARI • Complications - primary influenza pneumonia or secondary bacterial pneumonia, and myocarditis, particularly in children, elderly people and people with underlying chronic diseases • CFR: in general 1%, higher in older and chronically ill individuals, new pandemic strains also caused higher CFR
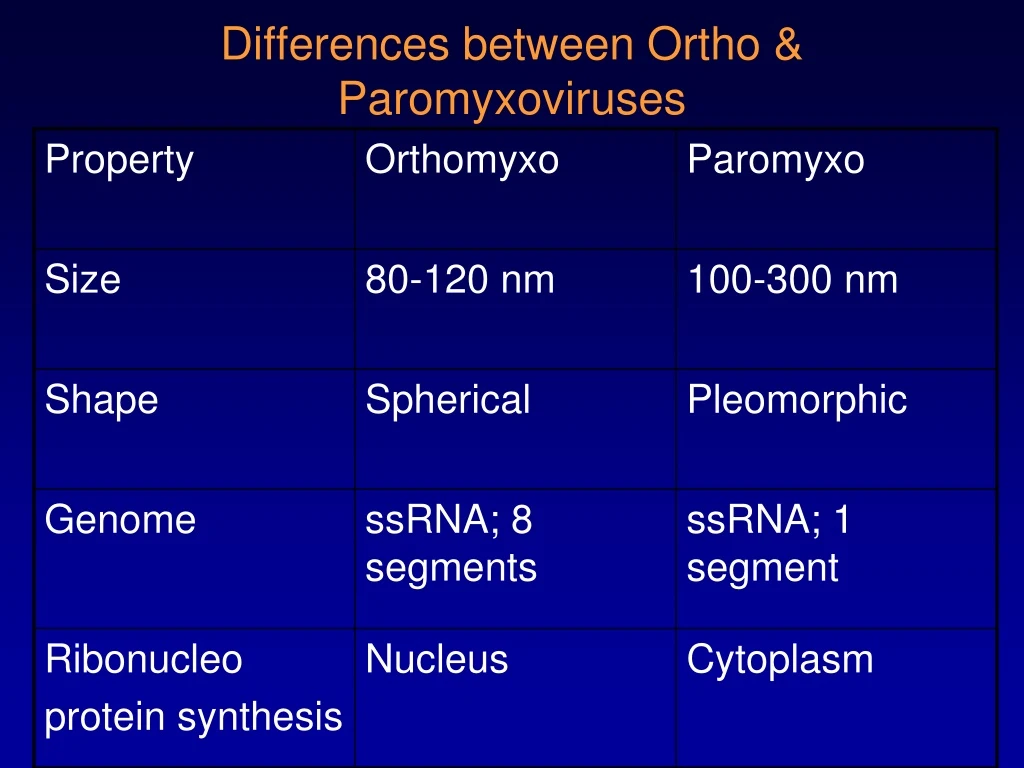
Influenza Virus - Structure • 80 – 120nm, Spherical • Single-stranded RNA Virus, 8 segmnts • RNA polymerase • Nucleocapsid is enclosed by an inner protein layer called matrix M protein • Outer lipid layer – derived from host cell membrane
HA - hemagglutinin NA - neuraminidase helical nucleocapsid (RNA plus NP protein) lipid bilayer membrane polymerase complex M1 protein ORTHOMYXOVIRUSES type A, B, C : NP, M1 protein sub-types: HA or NA protein
Antigenic classification • 3 influenza types: A, B, C ( Based on RNP & M protein) • type A: moderate/severe epidemics, affects humans and animals • type B: milder epidemics, affects only humans • type C: no epidemics; sporadic cases in humans • Influenza subtypes of type A determined by hemagglutinin (H) and neuraminidase (N)
ANTIGENIC VARIATION Antigenic drift - minor changes in either haemagglutinin or neuraminidase or both • Gradual change; regular; frequent intervals • Mutation in HA & NA genes • Periodic epidemics • Cross reacts with antisera to predecessor virus
Antigenic shift – Major changes in HA & NA or both • New subtypes • Abrupt & Drastic change • Results from gene reassortment between human and animal strains • Major epidemics & Pandemics • Antibodies to predecessor virus cannot neutralize new variants
Antigenic Changes of Influenza Virus • Type A: major change of hemagglutinin (H) and/or neuraminidase (N) resulting in new subtypes and pandemics • 4 pandemics in 19th century • 1918: subtype H1N1: severe pandemic, 20 million deaths • 1957: subtype H2N2: severe pandemic • 1968: subtype H3N2: moderate pandemic • 1977: subtype H1N1: mild pandemic • 1989; subtype H1N1; swine flu • 2009; subtype H1N1; • Minor antigenic change within the same subtype, associated with epidemics • Type B: no subtypes, only minor antigenic changes, associated with epidemics
Reservoir and Transmission • Reservoir: humans, animals (type A); • all human influenza A viruses infect avian species, • few antigenic subtypes of influenza A infect man and other animals (pigs and horses); • evidence that the viruses which caused pandemics originated from animals: swine strain (1918), avian strains (1957, 1968) • Transmission: airborne, through respiratory droplets • Seasonality: temperate regions: winter, tropics: often in the rainy season • Incubation period: 1-3 days • Communicability: 1-2 days before to 4-5 days after onset
where do “new” HA and NA come from? • 13 types HA • 9 types NA • all circulate in birds • pigs • avian and human
Where do “new” HA and NA come from- can ‘new’ bird flu directly infect humans? Bird flu H5N1?
Pathogenesis • Infection spreads from person to person via respiratory secretions, by airborne droplets or by contact with contaminated hands or surfaces. • Virus attaches to and infects the respiratory mucosal epithelial cells. • Progeny virions are soon produced and spread to adjacent cells, where the replicative cycle is repeated.
Influenza viruses cause cellular destruction and desquamation of superficial mucosa of the respiratory tract. • Viral damage to the respiratory tract epithelium lowers its resistance to secondary bacterial invaders. • Prominent systemic symptoms associated with influenza probably reflect the production of cytokines.
NORMAL TRACHEAL MUCOSA 3 DAYS POST-INFECTION 7 DAYS POST-INFECTION
DECREASED CLEARANCE • RISK BACTERIAL INFECTION • VIREMIA RARE
PULMONARY COMPLICATIONS • CROUP (YOUNG CHILDREN) • PRIMARY INFLUENZA VIRUS PNEUMONIA • SECONDARY BACTERIAL INFECTION • Streptococcus pneumoniae • Staphlyococcus aureus • Hemophilus influenzae
NON-PULMONARY COMPLICATIONS • myositis (rare, > in children, > with type B) • cardiac complications • recent studies report encephalopathy • 2002/2003 season studies of patients younger than 21 yrs in Michigan - 8 cases (2 deaths) • liver and CNS • Reye’s syndrome • peripheral nervous system • Guillian-Barré syndrome
LAB DIAGNOSIS Microscopy – Smears from nasopharyngeal secretions, nasal swab, centrifuged deposit of throat garglings • Direct immunofluorscence – Demonstration of viral antigens Culture - throat garglings • Amniotic cavity of chick embryo - amniotic fluid and allantoic fluid is tested for HA using Guinea pig & fowl RBC’s at RT & 4•C • Monkey kidney cell cultures
Serology • CFT • HAI test - • Serum diluted serially • Influenza virus suspension with 4HAunits added • Fowl RBC’s added • Highest dilution inhibiting HA – HAI titre
Treatment • Neuraminidase inhibitors are a new class of drugs used for the treatment of influenza. • They act by inhibiting the release of the virus from infected cells. This limits the infection by reducing the cell to cell spread of the virus. • They are about 70 – 90 % effective against both influenza A and influenza
Zanamivir (Relenza) – is administered by inhalation. • Oseltamivir (Tami flu) – is given orally. • Amantadine & Rimantadine inhibit viral uncoating of Influenza A virus. • They are effective only against influenza A virus and were widely used in the prevention and treatment of influenza A. But now, due to the development of resistance, their use is not recommended.
Prevention using Influenza Vaccines • Trivalent Inactivated Vaccine (TIV) – It is an inactivated vaccine prepared from the influenza viruses grown in embryonated eggs. • It is given by intramuscular injection in 2 doses separated by a month.
Live Attenuated Influenza Vaccine (LAIV) – It is a cold adapted vaccine containing temperature sensitive (ts) mutants of influenza A and B viruses. These mutant strains can replicate in the cooler temperature (33oC) of the nasal mucosa where it induces the production of secretory IgA antibodies, but not in the warmer (37oC) of the lower respiratory tract. • It is administered by nasal spray (Flu Mist