Download

1 / 16
160 likes | 184 Vues
Explore the rise of Extensive Drug Resistance in Multi-Drug Resistant Tuberculosis patients undergoing MSF's anti-TB programs in Abkhazia and Uzbekistan, analyzing rates, outcomes, and potential risk factors.

E N D
Development of extensive drug resistance in Multi-Drug resistant tuberculosis patients MSF anti-TB programmes in Abkhazia and Uzbekistan Authors: Cathy Hewison, Vinciane Sizaire, Helen Cox, Stobdan Kalon, Stefan Nieman and Jonathan Polonsky
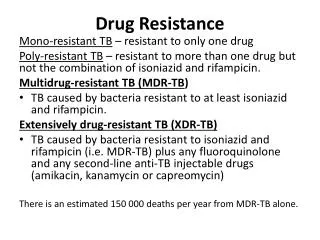
Some definitions • Multi-Drug Resistant (MDR) TB: Tuberculosis resistant to at least Isoniazid and Rifampicin • Extensive Drug Resistant (XDR) TB: MDR TB resistant as well to a fluoroquinolone (Oflo- or moxifloxacin) and a 2nd line injectable (Kanamycin or Capreomycin)
Settings • Abkhazia: • TB treatment as per WHO recommendation since 1998 • DST survey (Sept 2000 – March 2002): • MDR TB rate in new cases = 4% • MDR TB rate in re-treatment cases = 18.7% • Nov 2004: Green Light Committee approval • Aug 2001: 1st patient enrolled on MDR treatment • March 2003 – Sept 2005: Genotyping for the Long drug study
Settings • Nukus (Uzbekistan) • TB treatment as per WHO recommendation since 1998 with total coverage of Karakalpakstan achieved end of 2002 • DST survey in 2001: • MDR TB rate in new cases = 13% • MDR TB rate in re-treatment cases = 40% • Early 2003: Green Light Committee approval • Sept 2003: 1st patient enrolled on MDR treatment • Since May 2007: Genotyping study
Objectives • Primary objectives • To evaluate the XDR rate among MDR TB patients at diagnosis • To evaluate the rate of MDR TB cases who become XDR while on an adapted treatment • Secondary objectives • Amongst patients who become XDR during MDR treatment: • Identify the potential risk factors for developing XDR • Evaluate treatment outcomes • Define needs in further research from the current findings and eventual operational implications
Method • Retrospective cohort analysis of: • All MDR TB patients diagnosed at the 1st DST from the beginning of the project till end of December 2006, in order to evaluate the baseline XDR rate • All MDR TB patients enrolled on MDR treatment from the beginning of the project till end of December 2006, excluding those XDR at diagnosis, in order to evaluate the rate of MDR patients who become XDR while on treatment.
MDR TB diagnosis and follow-up • Diagnosis: • DST to all 1st line TB drugs, except Z, performed systematically in all M+, by MGIT in Abkhazia and by L-J in Nukus (MGIT will be available in June 2007) • DST to 2nd Line by L-J in all MDR patients identified • Follow-up: • Abkhazia: Culture/DST 1x/month during the IP and 1x/2 months during the CP • Nukus:Culture from M2, 1x/month till culture conversion then 1x/2 months. DST 1x/3 months
MDR TB patients management • Individual Treatment regimen: • IP: Minimum of 4 in Abkhazia, 5 in Nukus, 2nd Line TB drugs to which patient is susceptible, including an injectable for 4 to 6 months after culture conversion • CP: Same regimen but the injectable for 18 months • DOT • Comprehensive management of side-effects • Infection control measures in the hospital: • UV lights • Ventilation (difficult in the winter time) • High filtration masks for staff and visitors • Separation of the patients
MDR treatment outcomes • Treatment outcomes are reported according to WHO and international definitions: • Cure • Treatment completed • Death • Failure • Default • Still on treatment
Results: Baseline XDR rate among MDR TB patients • Abkahzia: • Sept 2000 – Dec 2006:147 MDR patients diagnosed • 6 (4.1%) were XDR at the time of diagnosis • Nukus: • Sept 2003 – Dec 2006: 428 MDR patients diagnosed • 7 (1.6%) were XDR at diagnosis
Results: Development of XDR TB during MDR treatment and outcomes
Results: Potential factors contributing to the development of XDR
Results: Discussion • 4.1% in Abkhazia and 1.6% in Nukus of MDR patients are XDR at the time of diagnosis • 13% in Abkhazia and 8% in Nukus of the MDR patients become XDR, while on a comprehensive MDR treatment • The only RF strongly associated with XDR development is the baseline resistance to 2nd Line drugs, confirmed by the multivariate analysis in Nukus (OR=6.02, p < 0.001) • We need also to look at the level of adherence to treatment as a RF
Conclusions • The apparition of XDR TB from a best practice MDR TB management is concerning • What are the mechanisms behind the XDR apparition? • True amplification • Re-infection • Multiple infections • Laboratory contamination
Conclusions • MDR strains genotyping through the treatment and molecular epidemiology are needed to: • Estimate the relative contribution of double infection, super-infection or true resistance amplification • Better define the RF that contribute to the development of XDR • Identify clusters, within families or within the hospital
Operational implications • If super-infection between patients during the stay in the hospital: • Urgent needs to improve infection control within the hospital • Consider ambulatory treatment from the beginning? • If family clusters • Aggressive active screening in all family members? • If true amplification • Use more aggressive treatment regimen, including 3rd Line TB drugs • Call for research on new drugs