Urea cycle and its defects
Urea cycle and its defects . Dr.S.Chakravarty MD. Learning objectives:. Explain the fate of carbon skeleton and nitrogen group of amino acids. Explain the ways of transport of nitrogen from various parts of the body to the liver

Urea cycle and its defects
E N D
Presentation Transcript
Urea cycle and its defects Dr.S.Chakravarty MD
Learning objectives: • Explain the fate of carbon skeleton and nitrogen group of amino acids. • Explain the ways of transport of nitrogen from various parts of the body to the liver • Describe the urea cycle and the enzymes involved in production of urea in the liver • Define and classify Hyperammonemias . List the enzymes deficient in various hyperammonemias and its clinical features
Catabolism of Amino acids • Amino group – NH3Formation of urea • Carbon skeletons – Formation of Glucose and Ketone bodies.
FATE OF THE CARBON SKELETONS Carbon skeletons are used for energy Glucogenic: TCA cycle intermediates or Pyruvate (Gluconeogenesis) Ketogenic: Acetyl CoA, Acetoacetyl CoA, or Acetoacetate
DIGESTION AND ABSORPTION • PROTEINS • Gastric juice ( acidity denatures proteins ) • Intestinal enzymes hydrolyze • AMINO ACIDS • Amino acid transporters Na+Amino acid symporter (can take up di and tri peptides ) • UPTAKE DEFECTS :- 1)Hartnups disease Long neutral amino acid transporter defect( Trp is not taken up Pellagra like symptoms as Trp Niacin is not formed ) 2)Cystinuria Basic amino acid transporter defect that also transports cysteineUrinary stones .Cystine forms Cystine by disulfide linkage (less soluble Stones )
EXCESS AMINO ACIDS ARE DEGRADED NOT STORED OVERVIEW OF AMINO ACID METABOLISM ENVIRONMENTORGANISM Bio- synthesis Protein Ingested protein 2 3 1 Recycling a AMINO ACIDS b c Degradation (required) c Purines Pyrimidines Porphyrins Nitrogen NH3 Carbon skeletons Urea (ketogenic) (glucogenic) pyruvate α-ketoglutarate succinyl-CoA fumarate oxaloacetate Used for energy acetoacetate acetyl CoA
NH3 is TOXIC
Why ammonia is toxic ? • Affects central nervous system • Alkalization of intracellular compartment • Disrupts oxidative phosphorylationATP depletion • Increased glutamate in Brain • Decreased Neurotransmitters – GABA – convulsions • Cerebral edema
Symptoms of AMMONIA toxicity • Flapping Tremor (Asterixis) • ( Correlate flapping tremor later on with Liver failure in Clinical medicine ) • Slurred Speech • Blurred Vision • COMA Death
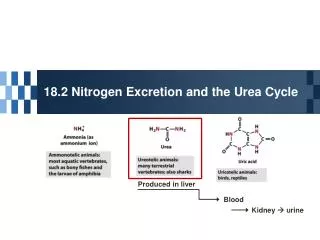
Metabolic fates of ammonia • Ammonotelic – Fishes • Lots of water available • Uricotelic – Reptiles and birds • Birds have to keep minimum body weight for flight • Ureotelic – Mammals
Adults degrade 1-2% of body protein daily Body Proteins 80-85% Amino acids 25% Catabolism UREA
Amino acids Sources of Amino Acids : Utilization of Amino acids: Synthesis of New proteins Formation of Nucleotides Formations of Porphyrins and Catecholamines Production of energy and Ammonia. • Exogenous – Diet • Endogenous – • Breakdown of muscle protein • Biosynthesis from intermediates of citric acid cycle.
Fate of Amino group 1) Reutilization: Glutamate and Glutamine are involved in recycling of amino acids. ATP ADP Glutamate + Ammonia Glutamine Glutamine Synthase • They are secreted by the peripheral tissues in form of glutamine which is taken up by hepatocytes where the NH3 is re-used for amino acid and nucleotide synthesis Glutamine Glutamate + Ammonia Glutaminase
2. Formation of amino acids from carbon skeletons require ammonia • Two important reactions are involved in fixing ammonia back to amino acids: • Reductive Amination: • Amino Transferases: • All non-essential amino acids except for tyrosine and cysteineare derived and are dependent on transamination from glutamate.
1. Reductive Amination : NAD(P)H NAD(P) Alpha ketoglutarate + Ammonia Glutamate Glutamate dehydrogenase 2. Transamination reaction: Alpha keto acid-1 Amino acid-1 Transaminase Alpha keto acid-2 Amino acid-2 PLP
UREA • Well balanced polarity (Quite uncharged because of amide nitrogen yet sufficiently soluble in plasma No transporter required ) • Non-Toxic AMMONIA ASPARTATE
CATABOLISM OF PROTEINS • UREA BIOSYNTHESIS IS DIVIDED INTO 4 STAGES:- • 1. TRANSAMINATION • 2. OXIDATIVE DEAMINATION • 3. AMMONIA TRANSPORT • 4. REACTIONS OF THE UREA CYCLE
TRANSAMINATION • DEF:-THE TRANSFER OF THE ALPHA-AMINO GROUP FROM ONE AMINO ACID TO A KETO ACID , RESULTING IN FORMATION OF A NEW AMINO ACID AND CORRESPONDING KETO ACID . • E.G :- REACTION CATALYZED BY ALANINE AMINOTRANSFERASE ALANINE PYRUVATE (AMINO ACID ) (CORRESPONDING KETO ACID ) α-KETOGLUTARATE GLUTAMATE (KETO ACID )(NEW AMINO ACID) ALT ALL TRANSAMINASES REQUIRE PLP (VIT B6) PLP
TRANSAMINATION Corresponding KA AA New AA KA
USES OF TRANSAMINATION • FIRST STEP OF CATABOLISM OF PROTEINS • SYNTHESIS OF NON-ESSENTIAL AMINO ACIDS and INTERCONVERSION OF AMINO ACIDS • REGENERATION OF TCA CYCLE intermediates
Sources of ammonia in the body • Aminoacids: • Transamination • Deamination • Transulfuration • Glutaminase • Gastrointestinal tract bacteria • Degradation of Amino sugars • Monoamine Oxidase • Pyrimidine catabolism
Nitrogen metabolism • Nitrogen part is toxic. Excreted in the form of either : • Ammonia – charged and alkaline. Excreted as ammonium ion in urine (3%) • Urea – Neutral molecule – Non toxic –( 80-85%) • Creatinine (3-4%) – constant in urine ( 1% of Creatine every day) • Uric acid – from Purines only !
Kaplan lecture notes USMLE step 1 Very important NH3 removal mechanism ( esp BRAIN)
Kaplan lecture notes USMLE step 1 WHY ALANINE ? NOT GLUTAMATE DIRECTLY (ALT) (AST) 2ND NITROGEN 1ST NITROGEN
Sources of ammonia in the body • Aminoacids: • Transamination • Deamination • Transulfuration • Glutaminase • Gastrointestinal tract bacteria • Degradation of Amino sugars • Monoamine Oxidase • Pyrimidine catabolism
Nitrogen metabolism • Nitrogen is Excreted in the form of either : • Ammonia – charged and alkaline. Excreted as ammonium ion in urine (3%) • Urea – Neutral molecule – Non toxic –( 80-85%) • Creatinine (3-4%) – constant in urine ( 1% of Creatine every day) • Uric acid – from Purines only !
Inter organ exchange of amino acids in post absorptive state (FASTING)
Inter organ exchange of amino acids in absorptive state (after feeding)
The Glucose alanine cycle ALT (Transamination) ALT (Transamination)
UREA • Well balanced polarity (Quite non polar because of amide nitrogen yet sufficiently soluble in plasma No transporter required ) • Non-Toxic AMMONIA ASPARTATE
Urea cycle High protein Diet Ammonia + Bicarbonate + ATP NAG – N-acetyl Glutamate CPS -1 activator Carbomyl Phosphate OrnithineTranscarbomylase Ornithine Citrulline Mitochondria Cytoplasm Arginosuccinatesynthase Aspartate Oxaloacetate Arginosuccinate ArginosuccinateLyase Fumarate TCA cycle Arginase Arginine Urea
Production of NAG: Acetyl Co-A + Glutamate N-acetyl Glutamate (NAG) N-acetyl glutamate synthase (NAGS) Arginine N-acetyl glutamate is the allosteric activator of Carbomyl phosphate synthase-1.
Urea cycle disorders • Hyperammonemia • Encephalopathy • Respiratory alkalosis • VOMITING • AVOIDANCE OF HIGH PROTEIN FOODS • INTERMITTENT ATAXIA • LETHARGY • SEVERE MENTAL RETARDATION
Symptoms of AMMONIA toxicity • Tremor • ( Correlate flapping tremor later on with Liver failure in Clinical medicine ) • Slurred Speech • Blurred Vision • COMA Death
Disorders of UREA cycle Hyperammonemia type -1 Hyperammonemia type -2 X-linked recessive Defect in OTC MC urea cycle defect Oroticaciduria present Cerebral oedema , coma and death. • Autosomal recessive • Defect in CPS- 1 • 1 in 200,000 • No oroticaciduria • Cerebral Oedema , coma and death . CAUSE OF OROTIC ACIDURIA Increased Carbamoyl phosphate spills out from mitochondia to cytosolPyrimidine synthesis Orotic acid
3. Citrullinemia : • Defect in arginosuccinatesynthase • Citrullinuria • Autosomal recessive 4. Arginosuccinicaciduria: • Defect in arginosuccinatelyase • Arginosuccinic acid blood, CSF, Urine 5. Hyperargininemia : • Diet without arginine • Defect in arginase enzyme
Treatment of Hyperammonemia: • Limit protein intake • Decrease bacterial source of ammonia – Antibiotics (Like Neomycin, Azithromycin)and Lactulose (purgative ) • Replace intermediates of urea cycle – ArginineCitrulline, Aspartate • Remove excess ammonia – Hemodialysis, sodium benzoate, phenyl acetate Very Important Very Important
Drugs • Lactulose – Acidification – conversion to NH4+ and induction of Purgation • Mainstay • Gut sterilization :-Neomycin/Azithromycinother antibiotics • Very Important • Combination of Sodium benzoate and Phenylacetate/Phenylbutyrate • Sodium benzoate + Glycine Hippuric acid excreted • Phenylacetate phenylacetyl glutamine excreted. (Phenylacetate conjugates with glutamine to form phenylacetylglutamine, which is excreted by the kidneys) • Rarely used
MCQ 1 Select the CORRECT answer . The first reaction in the degradation of the majority of common amino –acids involves participation of : • NAD + • Pyridoxal Phosphate • Thiamine Pyrophosphate(TPP) • FAD • NAD and TPP
MCQ 2 • After thorough investigations a man is diagnosed with oroticaciduria. To find out the cause of oroticaciduria which of the following investigations will you prefer? • A. ALP levels • B. vitamin b12 assay • C. FIGLU excretion assay • D. Peripheral smear • E. serum bilirubin