
Introduction
No. 010. The incidence of Inguinal Hernia occurrence at the time of Robotic Assisted Radical Prostatectomy and the outcomes of a policy of repair of all identified hernias. Associate Professor Laurence Harewood

Introduction
E N D
Presentation Transcript
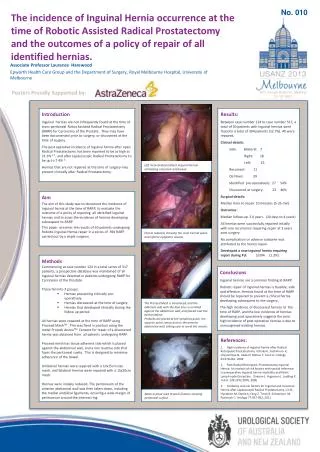
No. 010 The incidence of Inguinal Hernia occurrence at the time of Robotic Assisted Radical Prostatectomy and the outcomes of a policy of repair of all identified hernias. Associate Professor Laurence Harewood Epworth Health Care Group and the Department of Surgery, Royal Melbourne Hospital, University of Melbourne Posters Proudly Supported by: Introduction Inguinal hernias are not infrequently found at the time of trans-peritoneal Robot Assisted Radical Prostatectomy (RARP) for Carcinoma of the Prostate. They may have been documented prior to surgery, or discovered at the time of surgery. The post operative incidence of Inguinal hernia after open Radical Prostatectomy has been reported to be as high as 21.3% 1,2., and after Laparoscopic Radical Prostatectomy to be up to 7.4% 3.. Hernias that are not repaired at the time of surgery may present clinically after Radical Prostatectomy. Results: Between case number 124 to case number 517, a total of 50 patients with inguinal hernias were found in a total of 394 patients (12.7%). All were repaired. Clinical details: Side: Bilateral: 7 Right: 18 Left: 25 Recurrent: 11 De Novo: 39 Identified pre-operatively: 27 54% Discovered at surgery: 23 46% Surgical details: Median time to repair: 10 minutes (5-25 min) Outcomes: Median follow up: 2.0 years. (10 days to 4 years) All hernias were successfully repaired initially with one recurrence requiring repair at 2 years post surgery. No complication or adverse outcome was attributed to the hernia repair. Developed a new inguinal hernia requiring repair during FU: 5/394 (1.3%) Left incarcerated indirect Inguinal Hernia containing omentum and bowel. Aim The aim of this study was to document the incidence of inguinal hernia at the time of RARP, to evaluate the outcome of a policy of repairing all identified inguinal hernias and to asses the incidence of hernias developing subsequent to RARP. This paper presents the results of 50 patients undergoing Robotic Inguinal Hernia repair in a series of 394 RARP carried out by a single surgeon. Hernia reduced, showing the cord, hernial space and inferior epigastric vessels. • Methods • Commencing at case number 124 in a total series of 517 patients, a prospective database was maintained of all inguinal hernias detected in patients undergoing RARP for Carcinoma of the Prostate. • These fell into 3 groups: • Hernias presenting clinically pre-operatively. • Hernias discovered at the time of surgery. • Hernias that developed clinically during the follow up period. • All hernias were repaired at the time of RARP using Proceed MeshTM . This was fixed in position using the metal ProtackdeviceTM. Consent for repair of a discovered hernia was obtained from all patients undergoing RARP. • Proceed mesh has tissue adherent side which is placed against the abdominal wall, and a non reactive side that faces the peritoneal cavity. This is designed to minimise adherence of the bowel. • Unilateral hernias were repaired with a 10x15cm size mesh, and bilateral hernias were repaired with a 15x20cm mesh. • Hernias were initially reduced. The peritoneum of the anterior abdominal wall was then taken down, including the medial umbilical ligaments, ensuring a wide margin of peritoneum around the internal ring. Conclusions Inguinal hernias are a common finding at RARP. Robotic repair of inguinal hernias is feasible, safe and effective. Hernias found at the time of RARP should be repaired to prevent a clinical hernia developing subsequent to the surgery. The high incidence of discovered hernias at the time of RARP, and the low incidence of hernias developing post operatively suggests the prior high incidence of post operative hernias is due to unrecognised existing hernias. The Proceed Mesh is introduced, and the adherent side with the blue lines is unrolled against the abdominal wall, and placed over the hernial defect. Protacks are placed at the symphisis pubis, the superior pubic ramus and on the anterior abdominal wall, taking care to avoid the vessels. References: 1. High incidence of inguinal hernia after Radical Retropubic Prostatectomy. Ichioka K, Yoshimura K, Utsunomiya N, Ueda N, Matsui Y, Terai A. Urology 63:278-281, 2004 2. Post-Radical Retropubic Prostatectomy Inguinal Hernia: An analysis of risk factors with special reference to preoperative Inguinal hernia morbidity and Pelvic Lymph node Dissection. Stranne J, Hugosson J, Lodding P. J Urol 176:2072-2076, 2006 3. Incidence and risk factors for Inguinal and Incisional Hernia after Laparoscopic Radical Prostatectomy. Lin B, Hyndman M, Steele K, Feng Z, Trock B, Schweitzer M, Pavlovich C. Urology 77:957-962, 2011 Mesh in place with Protack fixation showing peritoneal surface .





